Creatine HCL vs Monohydrate: What the Research Shows
Which form is worth your money
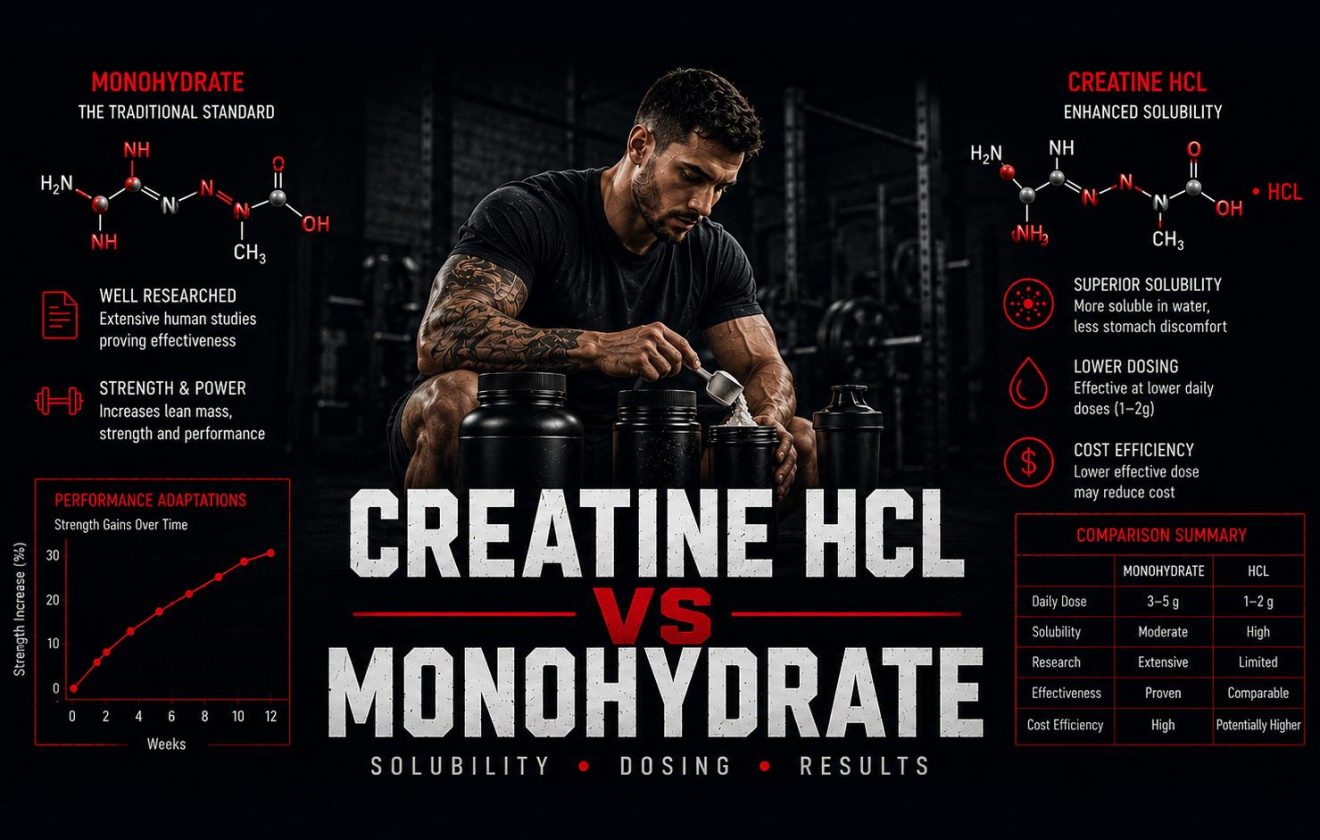
Creatine HCL is marketed as a superior form of creatine — more soluble, better absorbed, and effective at smaller doses than monohydrate. These claims have driven a significant price premium. This guide reviews the chemistry behind those claims, what the human trial data actually shows, and how creatine HCL compares to monohydrate on every measurable outcome.
Creatine HCL: Three Things to Know
What It Is
Creatine HCL is creatine bound to a hydrochloride salt. The HCL group lowers the pH of the compound, which substantially increases its solubility in water compared to monohydrate — approximately 38 times greater in laboratory testing.
What the Research Shows
Greater solubility does not automatically translate into greater efficacy. The only published head-to-head human trial comparing creatine HCL to monohydrate found no statistically significant difference in strength or body composition outcomes between the two forms at comparable doses.
Cost vs Evidence
Creatine HCL typically costs two to four times more per gram of creatine than monohydrate. Monohydrate has over 30 years of human trial data and is endorsed by the International Society of Sports Nutrition as the most evidence-backed creatine form available.
What This Article Covers
Covered
- What creatine HCL is and how it differs chemically from monohydrate
- The solubility argument: what it means and whether it matters
- Head-to-head human trial data on creatine HCL vs monohydrate
- Dosing comparison: how much HCL is needed versus monohydrate
- GI tolerability: does HCL actually solve monohydrate side effects
- Cost-per-dose analysis and practical considerations
- 5 key facts about creatine HCL for informed decision-making
Not Covered
- Product recommendations or brand comparisons
- Creatine cycling, loading protocol design
- Creatine for clinical populations (renal disease, pregnancy)
- Other creatine forms (ethyl ester, buffered, kre-alkalyn)
For the evidence framework used to evaluate supplement claims, see evidence-based supplements. For creatine monohydrate evidence summary, see performance supplements.
What Is Creatine HCL?
Creatine HCL is a salt formed by binding creatine to a hydrochloride molecule. The process lowers the pH of the resulting compound, producing a more acidic molecule that dissolves significantly more readily in water than creatine monohydrate. In laboratory solubility testing, creatine HCL dissolves at approximately 38 times the concentration of monohydrate at the same temperature and volume. This solubility advantage is real, reproducible, and the entire basis for the marketing claims made about the compound.
Creatine HCL entered the supplement market primarily through Con-Cret, a product launched around 2009 that positioned the form as a micro-dosed, high-absorption alternative to monohydrate. The marketing premise was straightforward: if creatine HCL is more soluble, it should be more bioavailable, and if it is more bioavailable, effective results should be achievable at smaller doses — typically claimed at one-quarter to one-tenth the standard monohydrate dose. This reasoning, while chemically plausible in principle, requires human pharmacokinetic data to validate — data that remains limited for creatine HCL.
How Creatine Works — The Baseline
Creatine in any form functions by increasing phosphocreatine stores in skeletal muscle. Phosphocreatine serves as a rapid energy buffer during high-intensity efforts lasting approximately 1 to 10 seconds — the energy system most relevant to resistance training, sprinting, and explosive sports. Increased phosphocreatine stores allow faster ATP regeneration between maximal efforts, which translates to additional reps at a given load, reduced fatigue during repeated sprints, and over time, greater training volume accumulation. This mechanism is well-established and applies regardless of which creatine salt reaches muscle tissue — what matters is the amount of creatine that is actually absorbed and stored.
For a full overview of how creatine fits into the supplement evidence hierarchy, the what are supplements guide covers the regulatory and evidence context, and the performance supplements guide covers the specific creatine monohydrate evidence base that creatine HCL is being compared against.
Chemical Structure and What It Means
By weight, creatine HCL contains approximately 78% creatine and 22% hydrochloride by molecular mass. Monohydrate contains approximately 88% creatine by weight. This means that per gram of product, monohydrate delivers more actual creatine than HCL. A label claiming “750 mg creatine HCL” provides roughly 585 mg of creatine — a detail relevant to dose comparisons and cost-per-effective-dose calculations.
Solubility: What It Means and Whether It Matters
The marketing argument for creatine HCL rests on the solubility-to-bioavailability chain: creatine HCL dissolves more readily in water → dissolved creatine is absorbed more efficiently in the gut → more creatine reaches muscle tissue → smaller doses produce equivalent results. Each step in this chain is plausible, but only the first has been directly measured and confirmed. The remaining steps require human pharmacokinetic and efficacy data that does not currently exist in the published literature for creatine HCL.
What Solubility Actually Predicts
Solubility determines how easily a compound dissolves in solution — in this case, in the aqueous environment of the gastrointestinal tract. For some compounds, poor solubility is a genuine absorption bottleneck: if a compound cannot dissolve, it cannot be absorbed across the intestinal wall. Creatine monohydrate is not one of those compounds. It has adequate solubility for gastrointestinal absorption at standard supplementation doses. The absorption ceiling for monohydrate is not solubility-limited — it is transport-limited, meaning the constraint is the capacity of intestinal creatine transporters, not the ability of the compound to dissolve. Increasing solubility 38-fold does not increase transporter capacity.
This does not mean creatine HCL’s solubility advantage is irrelevant — it does have practical implications for mixability in water and potentially for gastric discomfort at high doses. What it means is that the jump from “more soluble” to “more bioavailable at lower doses” requires evidence beyond solubility measurements, and that evidence has not been established.
GI Tolerability: Does HCL Solve the Monohydrate Problem?
One frequently cited advantage of creatine HCL is reduced gastrointestinal side effects compared to monohydrate. GI discomfort — bloating, cramping, loose stools — is associated with monohydrate primarily during the loading phase (20 g/day split into 4 doses over 5–7 days). The mechanism is osmotic: large amounts of undissolved or partially dissolved creatine draw water into the gastrointestinal tract. If creatine HCL dissolves more completely before reaching the lower GI tract, it may reduce this osmotic effect. This is a plausible hypothesis, but no published clinical trial has directly compared GI adverse event rates between monohydrate and creatine HCL in a controlled setting.
The practical context: monohydrate’s GI issues are dose-dependent and largely avoided by skipping the loading protocol and using a maintenance dose of 3–5 g/day. Most people who experience GI problems with monohydrate are loading at 20 g/day in large single doses. At standard maintenance dosing, GI issues are uncommon. The supplement labels guide covers how to evaluate side-effect claims in supplement marketing.
| Factor | Creatine Monohydrate | Creatine HCL |
|---|---|---|
| Solubility | 14 g/L at room temperature | ~500 g/L (approx. 38× more soluble) |
| Creatine by weight | ~88% creatine per gram | ~78% creatine per gram |
| Human trial volume | 300+ RCTs over 30 years | 1 published head-to-head human trial |
| Standard dose | 3–5 g/day maintenance | 1–2 g/day (label claim); no validated human dose |
| ISSN endorsement | Yes — most evidence-backed form | Not specifically endorsed |
| Typical cost/dose | Low (£0.04–0.08 per serving) | High (2–4× monohydrate per gram of creatine) |
Creatine HCL’s superior solubility is real and measurable. Its superiority in human performance outcomes has not been established. The solubility advantage does not automatically translate into a bioavailability advantage, and no published data confirms that creatine HCL produces superior muscle phosphocreatine saturation compared to monohydrate at any dose ratio.
Creatine HCL vs Monohydrate: What Human Trials Show
The central question is not whether creatine HCL dissolves more readily — it does — but whether that difference produces measurably better outcomes in humans. For monohydrate, the evidence base spans more than 300 randomized controlled trials accumulated over 30 years, covering strength, lean mass, sprint performance, cognitive function, and clinical applications. For creatine HCL, one published head-to-head human trial exists in the peer-reviewed literature.
The Spillane Study: The Only Head-to-Head Trial
The most cited human study on creatine HCL was published in the Journal of the International Society of Sports Nutrition. Researchers compared creatine HCL to monohydrate in resistance-trained men over a training period, measuring bench press and leg press strength, body composition, and various blood markers. The result: no statistically significant difference between creatine HCL and monohydrate in any primary outcome measure. Both groups improved similarly on strength and body composition. The study also found no significant difference in the blood markers measured, including creatinine — relevant because creatine supplementation of any form temporarily elevates serum creatinine, which can affect kidney function interpretation on bloodwork. The kidney markers guide covers this in detail.
The Spillane study used comparable creatine doses adjusted for the molecular weight difference between the two forms. Critics of the study note that the HCL dose may not have reflected the micro-dosing claims made by manufacturers — and this is a legitimate methodological point. However, the burden of proof rests on demonstrating that smaller doses of creatine HCL produce equivalent muscle phosphocreatine saturation to standard monohydrate doses. No published human trial has done this.
Bioavailability: What Is and Is Not Known
A compound’s solubility advantage translates into a bioavailability advantage only when absorption is genuinely solubility-limited. Creatine monohydrate at standard supplementation doses (3–5 g/day) is not absorbed at the limit of its solubility. The intestinal creatine transporter (SLC6A8) has finite capacity regardless of how much creatine is dissolved in the gut lumen. No published pharmacokinetic study in humans has demonstrated superior plasma creatine levels or superior muscle phosphocreatine accumulation from creatine HCL compared to equimolar doses of monohydrate. Until that data exists, the bioavailability advantage remains an extrapolation from in vitro solubility chemistry rather than a measured human outcome.
This gap between plausible mechanism and demonstrated human effect is the framework the evidence-based supplements guide uses to classify supplements — and it applies directly here. Creatine monohydrate has Tier 1 evidence (multiple large RCTs, consistent outcomes, ISSN endorsement). Creatine HCL has a plausible mechanism and one inconclusive human trial. That places it in a substantially lower evidence tier despite the higher price point.
Creatine and Recovery Context
One area where creatine’s evidence base is particularly strong — and where the form question is most relevant practically — is recovery between sessions. Monohydrate has well-documented effects on glycogen resynthesis, reduction of exercise-induced muscle damage markers, and satellite cell activity relevant to muscle repair. These effects are covered in the recovery supplements guide. Whether creatine HCL produces equivalent recovery benefits at smaller doses is not established in the literature. The conservative position is to use a dose that has been shown to saturate muscle phosphocreatine stores — which for monohydrate is 3–5 g/day over 28 days — rather than assume HCL’s solubility advantage allows a proportional dose reduction.
Dosing, Cost, and Who Might Consider Creatine HCL
Manufacturer recommendations for creatine HCL typically suggest 750 mg to 2 g per day — fractions of the 3–5 g monohydrate maintenance dose. These recommendations are based on the solubility and hypothesized bioavailability advantage, not on validated human dosing trials that confirm muscle phosphocreatine saturation at those levels. Without a pharmacokinetic study confirming equivalent creatine retention, the micro-dose claim requires the user to accept that the bioavailability argument holds in practice — which is not confirmed.
Cost Per Effective Dose
When comparing creatine HCL to monohydrate, cost-per-gram-of-creatine is the relevant metric — not cost-per-serving as listed on the label. Creatine HCL contains approximately 78% creatine by weight, versus monohydrate’s 88%. A 750 mg HCL serving provides roughly 585 mg of actual creatine. Monohydrate at 3 g/day provides 2.64 g of creatine. Even if HCL’s absorption were modestly superior, the cost differential — typically 2 to 4 times the price per gram of creatine — would need to be justified by a proportionally superior outcome that the current evidence does not demonstrate. For label-reading guidance on serving size and ingredient weight claims, see how to read supplement labels.
Who Might Have Reason to Consider HCL
Two scenarios are sometimes cited as legitimate use cases for creatine HCL over monohydrate: individuals who experience persistent GI discomfort even at monohydrate maintenance doses (not loading doses), and individuals who need to minimize fluid intake for competition-specific reasons and want the smallest dissolved volume per dose. Both are minority use cases. For the majority of recreational and competitive athletes, monohydrate at 3–5 g/day without loading produces full muscle phosphocreatine saturation within 28 days, causes no GI issues, and costs a fraction of creatine HCL.
For athletes subject to drug testing, creatine in any form is not prohibited. Creatine supplementation of any type temporarily elevates serum creatinine, which can produce abnormal-appearing eGFR values on bloodwork — a pattern that can concern clinicians unfamiliar with supplement use. The kidney markers guide covers how to interpret creatinine and eGFR in this context. The broader bloodwork context for athletes is covered at the bloodwork hub.
Monohydrate Dosing (Validated)
3–5 g/day for 28 days produces full muscle phosphocreatine saturation without loading. Supported by 300+ human trials. Loading at 20 g/day over 5–7 days achieves saturation faster but is not required and increases GI side effect risk.
Creatine HCL Dosing (Claimed, Not Validated)
Manufacturers recommend 750 mg to 2 g/day based on hypothesized superior bioavailability. No published human trial confirms these doses achieve equivalent muscle phosphocreatine saturation to monohydrate at 3–5 g/day.
5 Key Facts About Creatine HCL
- 1
Greater Solubility Does Not Mean Greater Efficacy
Creatine HCL’s 38-fold solubility advantage over monohydrate is real in laboratory conditions. Its translation into superior human performance outcomes is not demonstrated. Monohydrate’s absorption is not limited by solubility at standard supplementation doses — it is limited by intestinal transporter capacity, which is the same regardless of which salt form is dissolved in the gut.
- 2
The Only Head-to-Head Human Trial Found No Significant Difference
One published randomized controlled trial has directly compared creatine HCL to monohydrate in humans measuring performance outcomes. It found no statistically significant advantage for creatine HCL over monohydrate on strength or body composition. Until more comparative human trial data exists, claims of superiority are extrapolations from chemistry, not evidence-based conclusions.
- 3
The Micro-Dose Claim Has No Validated Human Pharmacokinetic Support
Manufacturer recommendations for creatine HCL at 750 mg to 2 g/day assume proportionally superior absorption relative to monohydrate. No published human pharmacokinetic study has measured plasma creatine concentrations or muscle phosphocreatine accumulation at these doses and confirmed equivalence to monohydrate at 3–5 g/day. The micro-dose claim is a hypothesis, not a validated dosing protocol.
- 4
Creatine HCL Delivers Less Creatine per Gram Than Monohydrate
By molecular weight, creatine HCL is approximately 78% creatine versus monohydrate’s 88%. Per gram of product, monohydrate delivers more actual creatine. This matters for cost-per-dose calculations: the higher sticker price per gram of creatine HCL is compounded by lower creatine content per gram of product, making the cost differential larger in practice than label prices suggest.
- 5
Monohydrate Has ISSN Endorsement; Creatine HCL Does Not
The International Society of Sports Nutrition’s position stand on creatine — the most comprehensive evidence review of creatine supplementation available — explicitly endorses creatine monohydrate as the most extensively studied and evidence-supported form. The ISSN position stand notes that no other creatine form has been demonstrated to be more effective than monohydrate. This assessment reflects the research landscape as of its most recent update and applies directly to the creatine HCL comparison.
Common Mistakes When Evaluating Creatine Forms
Equating Solubility With Bioavailability
The most common mistake in evaluating creatine HCL is treating the solubility advantage as equivalent to a bioavailability advantage. Solubility predicts absorption only when solubility is the limiting factor. For creatine at typical supplementation doses, absorption is transporter-limited, not solubility-limited. The chemistry argument for creatine HCL does not transfer directly into a measurable human outcome without pharmacokinetic evidence showing superior plasma or muscle creatine levels.
Taking Manufacturer Dosing Recommendations at Face Value
Creatine HCL micro-dose recommendations (750 mg to 2 g/day) are based on the unvalidated assumption that superior solubility produces proportionally superior absorption. No clinical dose-finding study for creatine HCL has determined the minimum effective dose for muscle phosphocreatine saturation in humans. Taking these recommendations as validated science rather than marketing extrapolation risks under-dosing creatine entirely, negating any potential benefit of the form. See supplement labels for how to identify unsupported dosing claims.
Using Creatine HCL to Avoid GI Issues From Monohydrate Loading
GI discomfort from creatine monohydrate is associated with high-dose loading protocols — typically 20 g/day split into four doses. At a maintenance dose of 3–5 g/day without loading, most users experience no GI side effects. Switching to creatine HCL to solve monohydrate GI issues without first trying a maintenance-only monohydrate protocol is solving a problem that often does not exist at lower doses, at 2–4 times the cost.
Ignoring the Bloodwork Context for Creatine Supplementation
Any form of creatine supplementation — monohydrate or HCL — temporarily elevates serum creatinine. This is a normal physiological response, not evidence of kidney stress in healthy individuals. However, it can produce eGFR values outside the normal range on routine bloodwork, which can create unnecessary concern. Athletes and clinicians should be aware of this when interpreting kidney function markers during creatine use. The kidney markers guide and the broader training context guide provide relevant background.
Research Sources
- Spillane M et al. “The effects of creatine ethyl ester supplementation combined with heavy resistance training on body composition, muscle performance, and serum and muscle creatine levels.” J Int Soc Sports Nutr, 2009 — PubMed
- Kreider RB et al. “International Society of Sports Nutrition position stand: safety and efficacy of creatine supplementation in exercise, sport, and medicine.” J Int Soc Sports Nutr, 2017 — PubMed
- Hultman E et al. “Muscle creatine loading in men.” Journal of Applied Physiology, 1996 — PubMed
- Rawson ES, Volek JS. “Effects of creatine supplementation and resistance training on muscle strength and weightlifting performance.” J Strength Cond Res, 2003 — PubMed
- Greenhaff PL et al. “Influence of oral creatine supplementation of muscle torque during repeated bouts of maximal voluntary exercise in man.” Clinical Science, 1993 — PubMed
- Antonio J, Ciccone V. “The effects of pre versus post workout supplementation of creatine monohydrate on body composition and strength.” J Int Soc Sports Nutr, 2013 — PubMed
Creatine HCL: The Verdict
Creatine HCL is a chemically distinct form of creatine with a measurable solubility advantage over monohydrate. It is not a fraudulent product and it is not dangerous. The problem is the gap between what can be measured in a test tube and what has been demonstrated in humans: greater solubility does not produce confirmed greater bioavailability, and greater bioavailability — if it exists — has not been shown to produce superior muscle phosphocreatine saturation at the micro-doses recommended by manufacturers.
Creatine monohydrate, by contrast, has three decades of human trial data, an ISSN position stand endorsement, and a cost-per-effective-dose that is a fraction of creatine HCL. For the vast majority of users, monohydrate at 3–5 g/day without a loading protocol achieves full muscle phosphocreatine saturation within 28 days, causes no GI issues, and costs significantly less. The remaining evidence gap does not justify a 2–4 times price premium for creatine HCL as a routine choice.
The decision changes only if a user has persistent GI intolerance at maintenance monohydrate doses — a minority case — and even then, this should be verified before switching rather than assumed. The evidence framework for making that kind of evaluation is covered across these guides:
This article is published for educational purposes only. It presents an evidence-based comparison of creatine HCL and creatine monohydrate based on available peer-reviewed research and published position statements. Nothing here constitutes medical advice, a product recommendation, or a purchasing recommendation of any kind. MuscleScience.org does not sell, supply, or endorse any supplement product or brand.
Creatine supplementation in healthy individuals is considered safe in the peer-reviewed literature at doses used in research. Individuals with pre-existing kidney conditions should consult a physician before using any creatine supplement. The temporary serum creatinine elevation from creatine supplementation is not evidence of kidney damage in healthy users — see the kidney markers guide for context.
This contributor writes under a pseudonym. The photograph above is a stylized portrait, not a real image of the writer. See our About page for details on our editorial team and anonymity policy.


