Growth Hormone Peptides: How GH Secretagogues Work and What Research Shows
How GH secretagogues actually work
Growth hormone peptides are compounds that stimulate the pituitary gland to release more of its own GH — they do not supply exogenous growth hormone. Understanding how growth hormone peptides differ from each other, which receptor each subclass targets, and what the evidence base actually contains is the starting point for reading any research claim about this compound class accurately.
Growth Hormone Peptides: Three Facts Before You Read Any Claim
These three facts define what growth hormone peptides are and how they work. Every claim about a specific compound in this class connects back to one or more of these points.
They Signal, Not Supplement
Growth hormone peptides do not contain or deliver GH. They signal the pituitary to release more of its endogenous GH through one of two receptor pathways. The magnitude of the GH response depends on the pituitary’s functional capacity, the somatostatin tone at the time of administration, and the specific receptor subclass the compound targets. A non-functioning or suppressed pituitary will not respond.
Two Distinct Receptor Subclasses
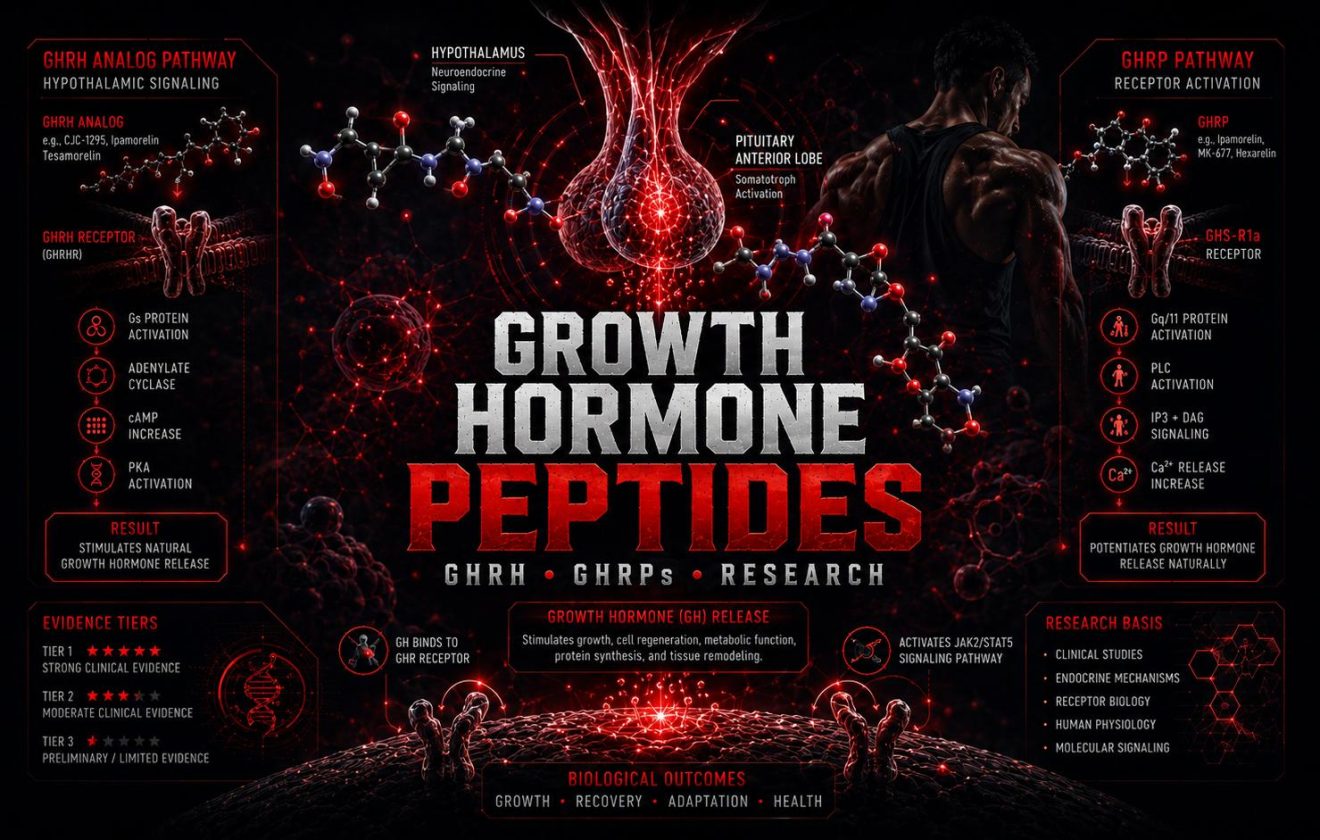
Growth hormone peptides split into two mechanistically separate groups. GHRH analogs bind the GHRH receptor on pituitary somatotroph cells. GHRPs bind the ghrelin receptor (GHS-R1a) at both the pituitary and hypothalamus. These receptor systems are complementary, not redundant — which is why combining compounds from each subclass amplifies the GH response beyond what either produces alone.
Evidence Is Not Uniform Across Compounds
Within growth hormone peptides, evidence quality ranges from small pharmacokinetic studies in healthy adults to animal-only data. Tesamorelin is FDA-approved for a specific indication and has human RCT data. Ipamorelin and most GHRPs have no published human efficacy trials for performance applications. Treating all compounds in this class as equally supported by research is one of the most consistent errors in how growth hormone peptides are described outside of clinical literature.
What This Guide Covers
Covered in This Guide
- How the GH axis works and where growth hormone peptides act within it
- The receptor distinction between GHRH analogs and GHRPs
- Key compounds in each subclass and their studied mechanisms
- What human pharmacokinetic and clinical data exists for each compound
- Evidence boundaries — what growth hormone peptides cannot do based on current data
- 5 common mistakes in how GH secretagogues are described
Not Covered Here
- GH replacement therapy (exogenous HGH) — different mechanism entirely
- IGF-1 directly — covered separately in the Research hub
- Dosing, reconstitution, or injection protocols
- Healing peptides (BPC-157, TB-500) — separate guide in this hub
- Non-peptide GH secretagogues such as MK-677 (ibutamoren)
Prerequisites. This guide assumes familiarity with the What Are Peptides guide and the Types of Peptides classification guide. For dosing math, see the Peptide Dosage Calculator.
This guide covers six topics on growth hormone peptides and how to evaluate the research on them.
How the GH Axis Works and Where Growth Hormone Peptides Act
Growth hormone is not released continuously. The pituitary secretes GH in pulses — typically 6 to 12 per day — with the largest pulse occurring during deep sleep. These pulses are controlled by two opposing hypothalamic hormones: growth hormone-releasing hormone (GHRH), which stimulates GH release, and somatostatin, which inhibits it. Growth hormone peptides act by amplifying the stimulatory side of this axis, by suppressing the inhibitory side, or both simultaneously depending on the subclass.
When GH is released into circulation, it travels to the liver and other peripheral tissues where it stimulates the production of insulin-like growth factor 1 (IGF-1). IGF-1 mediates most of the anabolic and tissue-remodeling effects attributed to GH — protein synthesis, lipolysis, cellular proliferation. Growth hormone peptides that successfully increase GH output will therefore indirectly elevate IGF-1, which is one reason IGF-1 is measured as a proxy for GH secretory status in clinical research on these compounds.
The GH-IGF-1 axis is subject to negative feedback at multiple points. Elevated IGF-1 signals the hypothalamus to increase somatostatin release and reduce GHRH secretion, limiting how much further GH the pituitary will produce. This feedback mechanism means that supraphysiological stimulation of GH release through growth hormone peptides does not produce indefinitely rising GH levels — the system self-limits. The magnitude of the ceiling depends on pituitary reserve and feedback sensitivity, both of which decline with age.
Growth hormone peptides act upstream of GH itself — they do not bypass this feedback system. A compound that maximally stimulates the GHS-R1a receptor will still produce a blunted response if somatostatin tone is high, if pituitary somatotroph reserve is depleted, or if the individual’s baseline GH output is already near their physiological ceiling. These variables are not controlled for in most research on growth hormone peptides and are rarely mentioned in non-clinical discussions of these compounds.
GHRH and Somatostatin
The hypothalamus governs GH release through two opposing peptides. GHRH (growth hormone-releasing hormone) drives pituitary somatotroph cells to release GH in pulses. Somatostatin suppresses GH release and blunts pituitary responsiveness. Growth hormone peptides in the GHRH analog subclass mimic GHRH; GHRPs partially suppress somatostatin release at the hypothalamic level, amplifying the net GH pulse.
Somatotroph Response
Pituitary somatotroph cells are the effector cells that actually release GH. Their response to growth hormone peptides depends on receptor density, intracellular cAMP levels triggered by GHRH-R activation, and concurrent calcium signaling from GHS-R1a activation. Pituitary reserve — the functional pool of somatotrophs — declines with age, explaining why older adults show smaller GH responses to secretagogue stimulation than younger subjects in pharmacokinetic studies.
IGF-1 Production
Released GH travels to the liver where it binds GH receptors and stimulates IGF-1 synthesis. Circulating IGF-1 is the primary mediator of GH’s anabolic effects on muscle, bone, and connective tissue. Because IGF-1 is more stable in circulation than GH (half-life hours vs minutes), it is used as a surrogate marker in clinical studies of growth hormone peptides. Elevated IGF-1 also feeds back negatively on hypothalamic GHRH and pituitary GH secretion.
Negative Feedback Loop
GH and IGF-1 both feed back to suppress further GH release — GH by stimulating hypothalamic somatostatin, IGF-1 by reducing pituitary sensitivity to GHRH. This regulatory loop limits the total GH output achievable through growth hormone peptides regardless of dose. It also explains why chronic administration of secretagogues may produce diminishing returns as negative feedback adapts to elevated GH-IGF-1 levels.
GH peptides vs exogenous GH. Exogenous recombinant GH bypasses all of this. It delivers GH directly into circulation regardless of pituitary state, somatostatin tone, or negative feedback. Growth hormone peptides cannot replicate supraphysiological GH levels achievable with exogenous injection — they are ceiling-limited by pituitary reserve and feedback. This distinction is foundational for interpreting any comparison between growth hormone peptides and GH replacement in research literature.
GHRH Analogs vs GHRPs: The Two Subclasses of Growth Hormone Peptides
Growth hormone peptides divide into two mechanistically distinct subclasses defined by their primary receptor target. GHRH analogs bind the GHRH receptor directly on pituitary somatotroph cells. GHRPs bind the ghrelin receptor (GHS-R1a) — expressed at both the pituitary and the hypothalamus. These are separate receptor systems that activate different intracellular cascades, which is why their effects are additive rather than redundant when combined.
GHRH analogs work by mimicking the body’s own GHRH signal. The natural GHRH peptide has a half-life of only a few minutes due to rapid cleavage by dipeptidyl peptidase IV (DPP-IV). GHRH analog growth hormone peptides such as CJC-1295, sermorelin, and tesamorelin are chemically modified at the cleavage site to resist DPP-IV, extending their active window from minutes to hours or, in the case of CJC-1295 with DAC, to days. This extended receptor engagement produces a more sustained elevation of baseline GH and IGF-1 rather than the sharp pulse characteristic of natural GHRH.
GHRPs work through the ghrelin receptor. Ghrelin is the endogenous ligand for GHS-R1a — a peptide hormone produced primarily in the stomach that promotes appetite and GH release. GHRP compounds structurally mimic ghrelin’s GH-releasing properties. Research has confirmed that GHRP-6’s mechanism of action at the pituitary requires intact endogenous GHRH signaling — GHRPs amplify the existing GH pulse rather than initiating one independently. In patients with hypothalamopituitary disconnection, GHRP-6 produces a blunted GH response, confirming its reliance on functional GHRH signaling.
Direct Pituitary Stimulation
These growth hormone peptides bind the GHRH receptor on somatotroph cells and trigger cAMP-mediated GH release. Modified to resist DPP-IV cleavage, they produce sustained baseline GH and IGF-1 elevation. Key compounds: CJC-1295 (with or without DAC), sermorelin, tesamorelin. CJC-1295 without DAC behaves like modified GHRH with hours-long activity; with DAC, it binds albumin for days-long activity and continuous baseline GH elevation.
Ghrelin Receptor Agonism
These growth hormone peptides bind GHS-R1a at both the pituitary and hypothalamus, amplifying the GH pulse through calcium-mediated signaling and partial somatostatin suppression. Key compounds: ipamorelin, GHRP-2, GHRP-6, hexarelin. Ipamorelin is the most receptor-selective — it stimulates GH release with minimal effect on cortisol or prolactin, unlike GHRP-2 and GHRP-6 which elevate both at research doses.
Receptor Synergy
Combining a GHRH analog with a GHRP produces a GH response substantially larger than either compound alone — an amplification documented in multiple pharmacokinetic studies. The mechanism is receptor complementarity: GHRH-R activation increases pituitary cAMP; GHS-R1a activation increases intracellular calcium and suppresses somatostatin. Both pathways converge on GH release but through independent intracellular routes, producing additive stimulation of growth hormone peptides’ primary endpoint.
Why ipamorelin is the reference GHRP. Among GHRP-class growth hormone peptides, ipamorelin was the first described as “selective” because it stimulates GH release without the cortisol, prolactin, or ACTH elevations seen with GHRP-2 and GHRP-6 at comparable doses. This selectivity profile — established in rat and sheep models in 1998 — is why ipamorelin became the standard reference compound for GHS-R1a research and why it is most frequently studied alongside GHRH analogs in combined-administration pharmacokinetic research.
4 Key Growth Hormone Peptides in Research
These four growth hormone peptides represent the most frequently studied compounds across both subclasses. They are selected for their documented pharmacokinetic data, their role in establishing receptor mechanisms, or their status as reference compounds in the clinical literature on GH secretagogues. Two are GHRH analogs; two are GHRPs. Together they illustrate how the subclass distinction maps to real differences in mechanism, half-life, and evidence quality.
The growth hormone peptides covered here are not the only compounds in their respective subclasses. Hexarelin, GHRP-2, tesamorelin, and modified sermorelin analogs are all referenced in the literature. These four are covered because they anchor the foundational research on mechanism and because they are the compounds most frequently cited when discussing the receptor complementarity between GHRH analogs and GHRPs.
CJC-1295
CJC-1295 is a synthetic GHRH analog modified at position 2 to resist DPP-IV cleavage. It exists in two forms: without DAC (drug affinity complex), which has a half-life of approximately 30 minutes and produces a pulse-like GH response; and with DAC, which covalently binds to circulating albumin, extending its half-life to approximately 8 days. The DAC form produces sustained, non-pulsatile GH and IGF-1 elevation rather than discrete pulses. Human pharmacokinetic data for CJC-1295 with DAC was published in 2006 in healthy adults, showing dose-dependent GH and IGF-1 increases persisting for up to 14 days post-injection. The DAC modification makes CJC-1295 one of the most pharmacokinetically distinct growth hormone peptides in this class — and also the one with the clearest divergence from natural pulsatile GH release.
Ipamorelin
Ipamorelin is a pentapeptide GHRP characterized in 1998 as the first growth hormone peptide in this class described as “selective” — meaning it stimulates GH release without significant co-stimulation of cortisol, prolactin, or ACTH at the doses studied. This selectivity distinguishes it from GHRP-2 and GHRP-6, which elevate cortisol and prolactin in parallel with GH. Ipamorelin acts at GHS-R1a with a half-life of approximately 2 hours in animal models. Human pharmacokinetic data in healthy volunteers has not been published in peer-reviewed literature. Its selectivity profile and minimal off-target receptor activity make it the standard reference GHRP in research protocols combining growth hormone peptides from both subclasses.
Sermorelin
Sermorelin is the synthetic form of the first 29 amino acids of endogenous GHRH — the biologically active fragment required for GHRH receptor binding. It was previously FDA-approved for use in pediatric GH deficiency diagnosis and short stature treatment, though this approval was withdrawn by the manufacturer in 2008 for commercial reasons rather than safety findings. Half-life is approximately 10–20 minutes. Sermorelin produces a physiologically pulsatile GH response that more closely mimics natural GHRH activity than DAC-modified growth hormone peptides. Because of its historical clinical use, it has the broadest regulatory context of any unapproved secretagogue currently discussed in performance research.
GHRP-6
GHRP-6 is one of the original synthetic GHRPs and among the most studied in clinical and diagnostic research contexts. It is a hexapeptide that acts at GHS-R1a and has been used in clinical studies to test pituitary GH reserve in GH-deficient patients. Research has confirmed that GHRP-6-stimulated GH release requires intact endogenous GHRH signaling — in patients with hypothalamopituitary disconnection, the GH response is blunted, establishing the mechanistic dependence of GHRPs on functional GHRH tone. Unlike ipamorelin, GHRP-6 substantially elevates cortisol and appetite at research doses. Its appetite-stimulating effect is the most pronounced of the commonly referenced growth hormone peptides and is mediated directly by GHS-R1a activity in the hypothalamus.
Tesamorelin: the approved exception. Tesamorelin is a GHRH analog growth hormone peptide with FDA approval for HIV-associated lipodystrophy. It has Phase III RCT data demonstrating visceral fat reduction in this specific population. Its evidence base is categorically different from any other growth hormone peptide discussed here — it represents the only compound in this class for which human efficacy, not just pharmacokinetics, has been demonstrated in a large controlled trial. No data supports extrapolating its lipodystrophy findings to healthy adults.
What Growth Hormone Peptides Cannot Do Based on Current Evidence
The most common failure in how growth hormone peptides are discussed is confusing what a compound mechanistically could do with what controlled research has demonstrated it does do in humans. The table below maps five frequently made claims against the actual evidence status for GH secretagogues in healthy adults.
These boundaries apply specifically to growth hormone peptides used outside of clinical GH deficiency contexts. The evidence base for secretagogues in diagnosed GH deficiency is wider than for performance use in healthy, eugonadal adults. No published RCT has evaluated a GHRP or GHRH analog for muscle mass, body composition, or performance endpoints in healthy adults without a defined hormonal deficit.
| Claim | What Evidence Exists | What Evidence Does Not Exist |
|---|---|---|
| Increases GH and IGF-1 | Documented in pharmacokinetic studies for CJC-1295, GHRP-6, and sermorelin in humans. GH and IGF-1 elevations are dose-dependent and reproducible. | No published data on how this elevation compares in magnitude to exogenous GH or what the functional ceiling is in healthy, eugonadal young adults. |
| Builds muscle mass | None in humans. Rodent studies show increases in lean mass with GHRP-6 and related compounds under specific conditions. | No controlled human trial has measured muscle mass or strength outcomes as a primary or secondary endpoint for any unapproved GH secretagogue. |
| Accelerates fat loss | Tesamorelin reduces visceral fat in HIV-associated lipodystrophy (Phase III RCT data). This is a specific pathological context. | No evidence for fat reduction in healthy adults. The lipolytic mechanism exists in theory via IGF-1, but has not been demonstrated under controlled conditions in this population. |
| Improves sleep quality | GH release is highest during slow-wave sleep. Compounds that amplify GH pulses may amplify nocturnal GH output. Observed anecdotally. | No human sleep study using polysomnography has evaluated any GHRP or GHRH analog in healthy adults with sleep architecture as a primary outcome. |
| Safer than exogenous GH | Self-limiting via negative feedback — physiological ceiling exists. No documented supraphysiological IGF-1 in published pharmacokinetic studies. | Long-term safety data does not exist for any unapproved growth hormone peptide in humans. “Ceiling-limited” is not equivalent to “established as safe” — the long-term effects of chronic GH pulsatile amplification have not been studied. |
Data refers to unapproved research compounds only. Tesamorelin is the exception — it has regulatory approval and RCT data for a specific indication. Swipe to scroll on mobile.
The pharmacokinetic-to-efficacy gap. Most human data for growth hormone peptides stops at pharmacokinetics — confirming that the compound raises GH and IGF-1, not that this elevation produces any specific functional outcome. A compound raising IGF-1 by 30% in a six-hour window does not, by itself, establish that muscle mass or recovery is improved. The functional endpoint has to be measured directly, and for most GH secretagogues it has not been.
5 Mistakes in How Growth Hormone Peptides Are Described
These five mistakes appear consistently in how growth hormone peptides are discussed outside of peer-reviewed research contexts.
- Mistake 1
Treating CJC-1295 With DAC and Without DAC as the Same Compound
CJC-1295 with DAC and CJC-1295 without DAC have different half-lives, different GH release profiles, and different implications for baseline IGF-1 elevation. Without DAC: half-life of ~30 minutes, pulsatile GH response, faster clearance. With DAC: half-life of ~8 days, continuous GH baseline elevation, fundamentally non-pulsatile pharmacology. Combining the two under the label “CJC-1295” conflates two distinct pharmacological profiles. The published human data — PMID 17018654 — refers specifically to the DAC formulation. Using this reference to support claims about the non-DAC form misrepresents the source.
- Mistake 2
Using GH Deficiency Research to Support Use in Healthy Adults
Most human research on growth hormone peptides — including diagnostic use of GHRP-6 and clinical use of sermorelin — was conducted in individuals with documented GH deficiency, pituitary disease, or a defined hormonal condition. Pituitary response to secretagogue stimulation differs substantially between GH-deficient and eugonadal individuals. Applying findings from GH-deficient populations — larger GH responses, documented functional benefits of GH normalization — to healthy adults assumes equivalence that has not been demonstrated and is mechanistically unlikely given the difference in baseline GH output and pituitary reserve.
- Mistake 3
Conflating IGF-1 Elevation with Muscle Growth
Growth hormone peptides that raise IGF-1 are frequently described as promoting muscle growth on that basis alone. IGF-1 is a mediator of anabolic signaling — it activates PI3K-Akt-mTOR and stimulates protein synthesis in skeletal muscle. But elevated circulating IGF-1 from secretagogue stimulation does not automatically translate to a net anabolic effect sufficient to produce measurable muscle mass change. The magnitude of IGF-1 elevation, its duration, the training status of the individual, and protein availability all determine whether an anabolic signal produces a structural outcome. None of these interactions have been studied for unapproved growth hormone peptides in controlled human trials.
- Mistake 4
Ignoring Cortisol and Prolactin Effects of Non-Selective GHRPs
GHRP-2 and GHRP-6 stimulate GH release but also produce measurable elevations in cortisol, prolactin, and ACTH at research doses. These are GHS-R1a-mediated effects that occur in parallel with GH stimulation, not separate from it. Discussing only the GH-raising properties of these compounds while omitting their cortisol response gives an incomplete picture of their pharmacology. Ipamorelin’s selectivity — its primary research distinction — is meaningful precisely because these co-stimulatory effects are absent or minimal. Treating all GHRPs as equivalent in their side-effect profile ignores the receptor pharmacology that defines each compound’s individual risk and benefit profile.
- Mistake 5
Describing MK-677 as a Growth Hormone Peptide
MK-677 (ibutamoren) is a GHS-R1a agonist — it acts on the same ghrelin receptor as GHRPs and produces GH and IGF-1 elevation through the same proximal mechanism. It is not a peptide. MK-677 is a non-peptide small molecule with oral bioavailability, a half-life of approximately 24 hours, and a completely different pharmacokinetic profile from any injectable GH secretagogue. It is frequently grouped with growth hormone peptides in performance research discussions. This conflation misleads on route of administration, half-life, molecular class, and the applicability of GH peptide research to predict MK-677’s behavior.
Primary Research Sources
Peer-reviewed references from PubMed used to verify receptor mechanisms, pharmacokinetic data, compound characterization, and evidence tier assessments in this guide.
- Ionescu M, Frohman LA. Pulsatile secretion of growth hormone (GH) persists during continuous stimulation by CJC-1295, a long-acting GH-releasing hormone analog. J Clin Endocrinol Metab. 2006;91(12):4792–4797. PMID 17018654
- Raun K, Hansen BS, Johansen NL, et al. Ipamorelin, the first selective growth hormone secretagogue. Eur J Endocrinol. 1998;139(5):552–561. PMID 9849822
- Popovic V, Leal A, Micic D, et al. GH-releasing hormone and GH-releasing peptide-6 for diagnostic testing in GH-deficient adults. Lancet. 2000;356:1137–1142. PMID 11030292
- Popovic V, Damjanovic S, Micic D, et al. Blocked growth hormone-releasing peptide (GHRP-6)-induced GH secretion and absence of the synergic action of GHRP-6 plus GH-releasing hormone in patients with hypothalamopituitary disconnection: evidence that GHRP-6 main action is exerted at the hypothalamic level. J Clin Endocrinol Metab. 1995;80(3):942–947. PMID 7883854
- Bowers CY, Momany FA, Reynolds GA, Hong A. Growth hormone (GH)-releasing peptide stimulates GH release in normal men and acts synergistically with GH-releasing hormone. J Clin Endocrinol Metab. 1990;70(4):975–982. PMID 2108187
Growth Hormone Peptides: Reading the Evidence on GH Secretagogues
Growth hormone peptides are not a single compound class with uniform evidence. GHRH analogs and GHRPs act on different receptor systems and produce different GH release profiles. Within each subclass, individual compounds differ in selectivity, half-life, and the breadth of their off-target receptor activity. CJC-1295 with DAC produces sustained non-pulsatile GH elevation; sermorelin produces physiological pulsatile stimulation; ipamorelin stimulates GH without co-elevating cortisol; GHRP-6 does not. These distinctions matter for reading any specific research claim about this compound class.
The evidence base for growth hormone peptides in healthy adults is narrow. Human pharmacokinetic data confirms that GH and IGF-1 rise in response to secretagogue stimulation. It does not confirm that this rise translates to muscle mass gain, fat loss, improved recovery, or any other functional performance outcome. Tesamorelin is the single exception — an FDA-approved GHRH analog with Phase III human efficacy data for a specific pathological indication that is not relevant to healthy adult use. Every other compound in this class operates on pharmacokinetic evidence extrapolated to functional claims that controlled research has not validated.
The guides in the Peptides hub apply this evidence framework to individual compounds and compound classes. The Types of Peptides guide provides the classification context for where growth hormone peptides sit relative to healing peptides, metabolic peptides, and cosmetic peptide types. The Peptide Dosage Calculator handles reconstitution math. For the broader evidence methodology underlying this type of analysis, see the Research hub.
- Peptides Hub — All Guides
- What Are Peptides? — Molecular Basis and Signaling
- Types of Peptides — Classification and Evidence Tiers
- Peptide Dosage Calculator
- Research Hub — Study Design and Mechanisms
- What Are Anabolic Steroids?
- Bloodwork and Health Hub
- About the Author — Ryan Hale
- Start Here — Site Navigation Guide
For Educational Purposes Only
This guide is produced for educational and harm-reduction purposes. MuscleScience.org does not sell, recommend, or endorse any compound. All content reflects a summary of published research and does not constitute medical advice.
Growth hormone peptides discussed in this guide are not approved for human use by regulatory agencies, with the exception of tesamorelin in its specific approved indication. Consult a licensed physician before making any decisions about GH-axis modifying compounds or any other pharmacological agents.
All author names are editorial pseudonyms. See the full site disclaimer and about page for editorial policy and anonymity disclosure.


