Nandrolone Steroids
The nandrolone family, explained
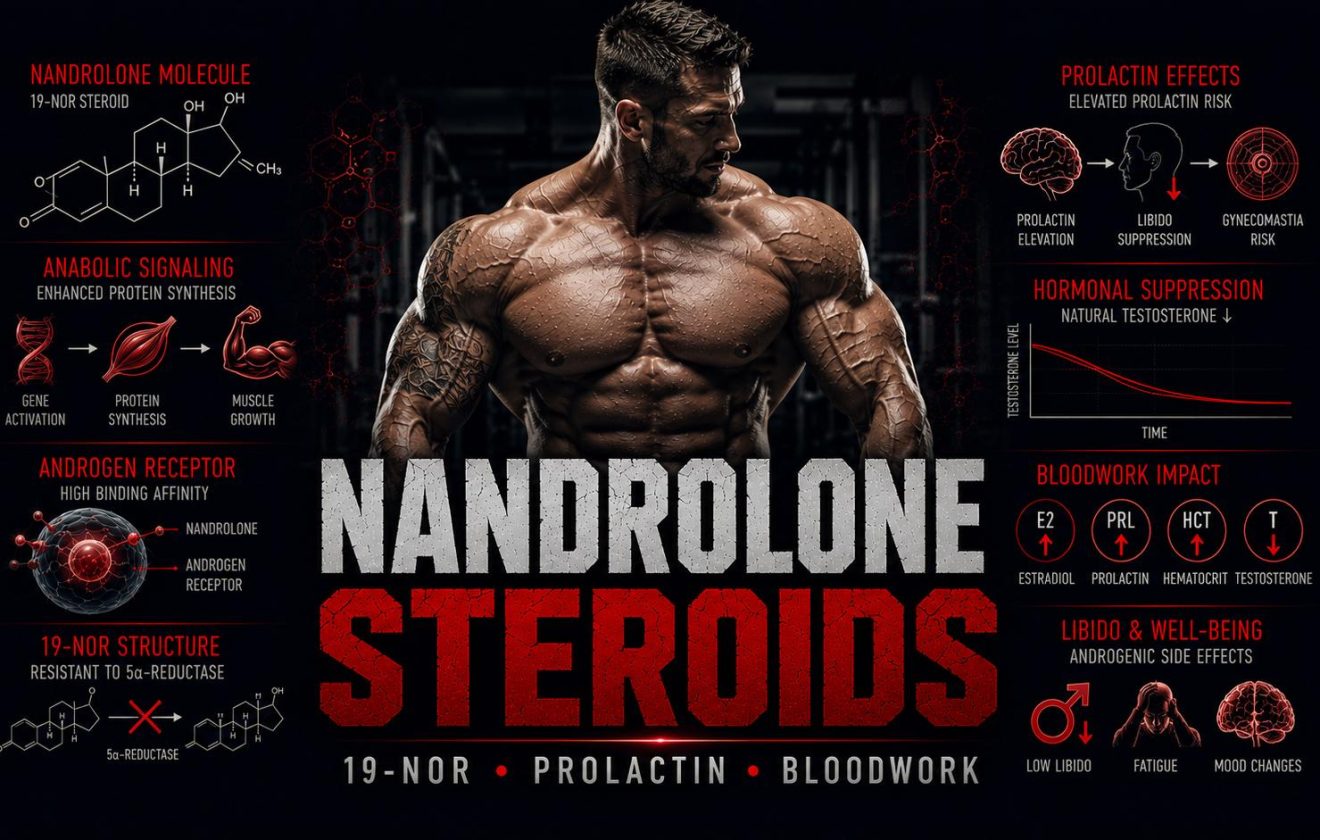
Nandrolone steroids are the most widely used 19-nor anabolic compounds — a structural class defined by the absence of a carbon atom at position 19 of the steroid backbone. This modification produces a pharmacological profile that is meaningfully distinct from testosterone-based and DHT-derived compounds: nandrolone steroids partially aromatize to estradiol, but less than testosterone; they convert via 5-alpha-reductase to a weaker androgen rather than a more potent one; and they interact with progesterone receptors in a way that drives one of the most clinically problematic effects associated with this class — prolactin elevation and its consequences for libido and sexual function.
Understanding nandrolone steroids requires understanding all three of these mechanisms simultaneously. The partial aromatization, the progestogenic activity, and the 5AR conversion pathway each contribute to a bloodwork and side-effect profile that cannot be predicted from testosterone pharmacology alone. This guide covers the 19-nor structural basis of nandrolone steroids, the main compounds in this class, what they do to key bloodwork markers, and the most common harm-reduction failures that occur when users apply testosterone-specific assumptions to nandrolone-based protocols.
Three Things That Define Nandrolone Steroids
Progestogenic Activity
Nandrolone steroids bind to progesterone receptors. Combined with elevated prolactin, this drives the libido and erectile dysfunction pattern known as “Deca dick” — one of the most discussed adverse effects specific to this compound class.
Partial Aromatization
Nandrolone steroids aromatize to estradiol at roughly 20% the rate of testosterone. Estradiol monitoring is still required — the conversion is real — but estrogen-related effects are generally less pronounced than on equivalent testosterone doses.
Severe HPTA Suppression
Nandrolone steroids suppress LH and FSH completely and persistently. Recovery after stopping is slower than with testosterone esters. The combination of progestogenic activity and depot release extends suppression well beyond the last injection date.
What This Guide Covers
Covered Here
- The 19-nor structural modification explained
- Why 5AR conversion works differently here
- Progestogenic activity and prolactin
- Main nandrolone steroids — profiles and distinctions
- Trenbolone as a separate 19-nor class
- 6 key bloodwork effects
- Bloodwork comparison table
- 5 common harm-reduction mistakes
- Blood Tests Before Steroids: 7 Markers to Check — the 7-marker baseline panel to run before starting
Not Covered Here
- Specific dosing protocols or cycle structure
- Dopamine agonist selection (cabergoline)
- PCT protocols in detail
- Fertility preservation strategies
- Legal sourcing or purchasing guidance
- Brand or vendor comparisons
Foundation: What Are Anabolic Steroids. Route context: Injectable vs Oral Steroids. Testosterone context: Testosterone Steroids.
What Are Nandrolone Steroids — The 19-Nor Structural Basis
The designation “19-nor” refers to the absence of a methyl group at carbon position 19 of the steroid skeleton. In testosterone, this carbon contributes to the androgenic character of the molecule in specific tissues. Its removal in nandrolone steroids produces three pharmacologically significant changes: the compound becomes a weaker substrate for the aromatase enzyme, it converts via 5-alpha-reductase to dihydronandrolone rather than DHT — a less potent androgen — and it acquires meaningful affinity for the progesterone receptor. These three differences from testosterone define the entire nandrolone steroids risk and monitoring framework.
The reduced androgenic activity in scalp and prostate tissues is a direct consequence of the 5AR conversion pathway producing a weaker metabolite. Users who experience significant hair loss or prostate symptoms on testosterone often find nandrolone steroids produce less of these effects at comparable androgenic doses — because the metabolite competing for those tissue receptors is dihydronandrolone, not DHT. This is frequently cited as an advantage of the class. The tradeoff is the progestogenic activity and prolactin pathway that testosterone does not carry.
Nandrolone steroids are among the most studied injectable anabolic compounds in clinical research — nandrolone decanoate has been used in HIV wasting, aplastic anemia, osteoporosis, and renal failure contexts with documented clinical outcomes. This clinical data provides a meaningful evidence base for understanding the compound’s actual pharmacological profile, which differs substantially from anecdotal community descriptions in several important respects.
Why 5AR Conversion Is Different With Nandrolone Steroids
When testosterone encounters 5-alpha-reductase in tissues like the scalp, prostate, and skin, it converts to DHT — a more potent androgen that drives androgenic effects in those tissues. When nandrolone steroids encounter the same enzyme, conversion produces dihydronandrolone — a compound with significantly lower androgenic potency than DHT and lower receptor affinity. This means 5-alpha-reductase inhibitors like finasteride, which reduce DHT by blocking 5AR, can paradoxically worsen the androgenic burden on a nandrolone steroids cycle: by reducing DHT, they reduce the competition for androgen receptors and allow nandrolone itself — which is more androgenic than dihydronandrolone — to dominate those receptors. This is the opposite of the effect finasteride produces on a testosterone cycle.
Nandrolone Steroids — Major Compounds in the 19-Nor Class
The 19-nor class contains several compounds beyond nandrolone itself. Trenbolone is also a 19-nor steroid but has a substantially different pharmacological profile — it does not aromatize at all, is significantly more androgenic and progestogenic than nandrolone steroids, and carries a distinct set of cardiovascular and CNS risks. It is covered separately below. The primary nandrolone steroids in clinical and performance discussion are nandrolone decanoate and nandrolone phenylpropionate.
Nandrolone Decanoate (Deca-Durabolin)
Injectable — Half-life 6–12 daysThe most widely used of the nandrolone steroids. Long-ester injectable requiring weekly or biweekly injection for stable blood levels. Clinically documented in multiple therapeutic contexts. Slow onset — blood levels take several weeks to stabilize and several weeks to fall after stopping. HPTA suppression persists significantly longer than with testosterone esters of equivalent half-life due to progestogenic contribution.
Nandrolone Phenylpropionate (NPP)
Injectable — Half-life 2–4 daysShort-ester nandrolone steroid requiring more frequent injection — typically every 2–3 days. Reaches peak concentration faster than decanoate and clears more quickly after stopping. Provides more flexibility to adjust dose or stop and allows faster recovery initiation. Identical pharmacological profile to decanoate — the ester controls kinetics only, not the compound’s activity.
Trenbolone Acetate
Injectable — Half-life ~2 days19-nor compound but pharmacologically distinct from nandrolone steroids. Does not aromatize. Extremely high androgenic and anabolic rating relative to testosterone. Strong progestogenic activity. Associated with cardiovascular strain, night sweats, sleep disruption, and aggressive CNS stimulation. Among the highest-risk injectable compounds in performance discussion. Short ester allows faster clearance if adverse effects appear.
Trenbolone Enanthate
Injectable — Half-life 5–7 daysLong-ester version of trenbolone. Identical pharmacological activity to the acetate form — the ester changes only injection frequency and depot duration. Less popular in harm-reduction contexts precisely because slower clearance means adverse effects persist longer after stopping. The shorter ester is generally recommended when trialing a compound for the first time.
Trenbolone is 19-nor but not nandrolone. The two share the structural class but differ in aromatization profile, androgenic potency, cardiovascular impact, and CNS effects. Applying nandrolone steroids risk assumptions to trenbolone — or vice versa — produces significantly inaccurate expectations. They require separate monitoring frameworks and separate risk assessment.
Nandrolone Steroids, Prolactin, and Sexual Function
The progestogenic activity of nandrolone steroids is the mechanism behind the most discussed adverse effect in this class: the complex of low libido, erectile dysfunction, and sexual dysfunction collectively known as “Deca dick.” This is not a single-cause phenomenon — it emerges from the interaction of several simultaneous hormonal changes that nandrolone steroids produce in ways testosterone does not.
Progesterone receptor activity from nandrolone steroids stimulates prolactin secretion from the pituitary. Prolactin — primarily known as the hormone regulating lactation — also directly suppresses dopaminergic tone in the hypothalamus and reduces sexual motivation at elevated levels. Simultaneously, nandrolone steroids suppress LH and FSH, eliminating endogenous testosterone production. The result is a hormonal environment with elevated prolactin, absent endogenous testosterone, low DHT (from the weak 5AR metabolite), and progestogenic receptor activity — a combination that consistently impairs sexual function.
Prolactin monitoring is mandatory on any cycle involving nandrolone steroids. Dopamine agonists — primarily cabergoline — are used clinically and in harm-reduction contexts to suppress prolactin elevation when it produces symptomatic sexual dysfunction. The decision to use cabergoline requires confirmed elevated prolactin via bloodwork, not symptom-only assessment — symptoms of low dopamine can mimic prolactin elevation and require laboratory confirmation to distinguish.
- Prolactin elevated via progestogenic receptor activity
- LH and FSH suppressed — no endogenous testosterone
- 5AR metabolite (dihydronandrolone) is weak androgen
- Partial aromatization — some estradiol present
- Progesterone receptor occupancy sustained by depot
- Dopaminergic tone suppressed by prolactin
- Prolactin not directly elevated
- LH and FSH suppressed — no endogenous testosterone
- 5AR metabolite is DHT — potent androgen
- Full aromatization — significant estradiol production
- No progesterone receptor activity
- Dopaminergic tone unaffected directly
Running testosterone alongside nandrolone steroids is the standard harm-reduction recommendation for partially counteracting the low-DHT and low-testosterone environment. Adding a testosterone base provides endogenous-like androgen receptor occupancy that partially offsets the sexual function suppression. It does not eliminate the prolactin risk — that requires bloodwork and, if indicated, pharmacological management.
6 Key Bloodwork Effects of Nandrolone Steroids
- 1
Prolactin — The Class-Defining Bloodwork Marker
Prolactin elevation is the bloodwork finding most specific to nandrolone steroids. It occurs via progestogenic receptor activity in the pituitary rather than through estrogen-driven mechanisms. Elevated prolactin is not always symptomatic — significant lactation or galactorrhea at performance doses is uncommon in men — but elevated prolactin in the context of suppressed testosterone and low DHT consistently produces the sexual dysfunction profile associated with this class. Prolactin should be measured pre-cycle and again 4–6 weeks into any nandrolone cycle. A dopamine agonist (cabergoline) is indicated when prolactin rises above the normal reference range with accompanying symptoms. See Bloodwork & Health hub.
- 2
LH and FSH — Complete Suppression, Slow Recovery
Nandrolone steroids suppress LH (luteinizing hormone) and FSH (follicle-stimulating hormone) to undetectable levels — the same HPTA shutdown that testosterone produces. The critical distinction is recovery time. The progestogenic activity of nandrolone steroids contributes to suppression independently of the androgen receptor pathway, meaning suppression persists longer after the last injection than testosterone ester pharmacokinetics alone would predict. Long-ester nandrolone decanoate cycles have among the slowest post-cycle HPTA recovery timelines in the injectable compound class. See TRT & Hormones hub.
- 3
Estradiol — Partial Aromatization Requires Monitoring
Nandrolone steroids aromatize at approximately 20% the rate of testosterone. Estradiol rises — but less dramatically than on equivalent testosterone doses. Estradiol monitoring is still required. When nandrolone steroids are combined with a testosterone base (the standard harm-reduction approach), the testosterone component produces its full aromatization independently, making estradiol management the same as any testosterone cycle. The nandrolone contribution to estradiol is additive but secondary. See Estradiol Before Steroids.
- 4
HDL Cholesterol — Moderate to Significant Suppression
Nandrolone steroids suppress HDL cholesterol via androgen receptor-mediated lipase activity — the same mechanism as other injectable anabolic compounds. The degree of suppression is generally less severe than with oral 17aa compounds but clinically meaningful at performance-range doses. Combined nandrolone and testosterone cycles compound the cardiovascular lipid burden. Lipid panels before and during use remain mandatory. Dose, duration, and individual baseline all affect the degree of HDL suppression significantly. See Lipid Panel: HDL, LDL, Triglycerides.
- 5
Hematocrit — Meaningful Elevation
Injectable nandrolone steroids stimulate erythropoiesis and produce hematocrit elevation comparable to testosterone esters. This is one of the less frequently discussed cardiovascular risks specific to long nandrolone cycles — hematocrit elevation persists as long as the compound is active, and with long-ester decanoate, active levels are sustained for an extended period after the last injection. Hematocrit above 52–54% significantly elevates thromboembolic risk. CBC monitoring during cycle is required. See Hematocrit & Hemoglobin (CBC).
- 6
PSA — Lower Androgenic Impact Than Testosterone
Because 5-alpha-reductase converts nandrolone to the weaker dihydronandrolone in prostate tissue rather than DHT, the direct androgenic stimulus to the prostate is lower than on equivalent testosterone doses. PSA elevation on nandrolone steroids cycles is generally less pronounced than on testosterone. However, PSA monitoring remains appropriate — particularly for men over 35, those with elevated baseline PSA, or those adding testosterone alongside nandrolone steroids. Absence of strong androgenic effect is not the same as absence of any androgenic effect.
Nandrolone Steroids — Bloodwork Impact by Marker
The table below reflects directional bloodwork changes for nandrolone steroids at performance doses. Combined testosterone-nandrolone cycles alter the estradiol and DHT columns significantly — testosterone contributions operate independently and add to the total hormonal exposure.
| Marker | Direction | Notes |
|---|---|---|
| Prolactin | Elevated — class-specific | Via progesterone receptor activity; monitor from week 4 |
| LH / FSH | Suppressed to zero | HPTA shutdown; recovery slower than testosterone due to progestogenic suppression |
| Estradiol | Mildly elevated | Aromatization ~20% of testosterone rate; monitoring required |
| HDL Cholesterol | Suppressed | Moderate — less than oral 17aa compounds; worse on combined cycles |
| LDL Cholesterol | May rise | Dose and duration dependent |
| Hematocrit | Elevated | Erythropoietic stimulation; persists through depot duration |
| AST / ALT | Minimal change | Injectable — no first-pass hepatic stress |
| PSA | Mild or no elevation | 5AR metabolite is weaker than DHT — lower prostate androgenic stimulus |
| Free Testosterone | Suppressed (endogenous) | HPTA shutdown eliminates endogenous production entirely |
Pre-cycle baseline for prolactin is frequently skipped and frequently regretted. Without a baseline value, elevated on-cycle prolactin cannot be distinguished from a pre-existing elevation. See Bloodwork & Health hub for full pre-cycle panel guidance.
5 Critical Mistakes With Nandrolone Steroids
- Mistake
Not Monitoring Prolactin Before or During the Cycle
Prolactin is the bloodwork marker most specific to nandrolone steroids and the most consistently skipped. Users who do not establish a pre-cycle prolactin baseline cannot distinguish a compound-driven elevation from a pre-existing one. Some individuals have elevated prolactin before any compound use — from a pituitary microadenoma, dopamine-affecting medications, or other causes. Treating symptomatic prolactin elevation with cabergoline without confirmed laboratory elevation is inappropriate and avoidable. Prolactin is a standard add-on to any pre-cycle bloodwork panel and costs no more than any other line item. See Bloodwork & Health hub.
- Mistake
Using Finasteride to Reduce Androgenic Effects on a Nandrolone Cycle
5-alpha-reductase inhibitors are counterproductive on nandrolone steroids cycles — not neutral. Finasteride works by blocking the enzyme that converts testosterone to DHT in tissue. When applied to nandrolone steroids, it blocks conversion to dihydronandrolone — a weak androgen — while leaving nandrolone itself available to occupy androgen receptors in scalp and prostate tissue. The result is more nandrolone, not less, competing at those receptors. The compound that replaces DHT in that tissue is more androgenic than the metabolite that was blocked. Finasteride is appropriate for testosterone-only cycles; it is contraindicated for harm-reduction purposes on nandrolone-based protocols.
- Mistake
Stopping a Long Ester Nandrolone Cycle Without Accounting for Depot Duration
Nandrolone decanoate has a half-life of 6–12 days. Full clearance requires multiple half-lives — meaning meaningful blood levels persist for 4–6 weeks after the last injection. Users who stop the compound expecting rapid recovery are consistently surprised by prolonged HPTA suppression and slow post-cycle normalization. This is compounded by the progestogenic suppression pathway, which operates independently of compound clearance through the androgen receptor. Planning a recovery timeline for nandrolone decanoate cycles requires explicitly accounting for depot duration — starting the recovery window from compound clearance, not last injection date.
- Mistake
Running Nandrolone Steroids Without a Testosterone Base
The standard harm-reduction recommendation for nandrolone steroids includes concurrent testosterone for a specific pharmacological reason: nandrolone steroids eliminate endogenous testosterone, their 5AR metabolite (dihydronandrolone) is a weak androgen, and prolactin elevation further suppresses sexual function. Without exogenous testosterone providing androgen receptor occupancy, the hormonal environment is significantly androgen-deficient at tissue level despite the presence of nandrolone. Sexual dysfunction in this setting is predictable. The testosterone-alongside-nandrolone approach is not a cultural convention — it reflects the compound’s actual pharmacological requirements for maintaining basic androgenic function at tissue level.
- Mistake
Assuming Lower Androgenic Risk Means Lower Overall Risk
Nandrolone steroids produce less androgenic effect in hair and prostate tissue than testosterone at equivalent anabolic doses — this is a real pharmacological distinction. It does not mean the compound is lower risk overall. Prolactin elevation, persistent HPTA suppression, HDL suppression, hematocrit elevation, and the extended recovery timeline after long-ester cycles represent a meaningful cumulative burden. Users who approach nandrolone steroids with reduced monitoring intensity because it is “not as androgenic as testosterone” miss the class-specific risks that are absent from testosterone entirely. The risk profile of nandrolone steroids is different from testosterone — not lower.
Authoritative Sources
- NCBI StatPearls — Anabolic Steroids: Pharmacology, Classification, Monitoring, and Adverse Effects
- PubMed — Nandrolone Decanoate: Pharmacological Properties and Therapeutic Use in Osteoporosis
- PubMed — Hyperprolactinemia and Male Sexual Function: Erectile Dysfunction and Sexual Desire
- PubMed — Effects of Androgenic-Anabolic Steroids on Apolipoproteins and Lipoprotein(a)
- Endocrine Society — Hypogonadism in Men: Testosterone and HPTA Clinical Context
- MedlinePlus — Anabolic Steroids: Health Risks Overview
Nandrolone Steroids — What the Pharmacology Actually Requires
Nandrolone steroids occupy a distinct position in the injectable anabolic compound landscape — not because they are safer than testosterone, but because their risk profile runs through entirely different mechanisms. The prolactin pathway, the slow HPTA recovery, the weak 5AR metabolite, the progestogenic receptor activity — none of these apply to testosterone. Users who approach nandrolone steroids with a testosterone-adapted monitoring framework miss the class-specific markers that matter most.
A responsible bloodwork approach to nandrolone steroids begins with pre-cycle baselines for prolactin, LH, FSH, estradiol, HDL, hematocrit, and PSA. On-cycle monitoring at 4–6 weeks covers prolactin, estradiol, and hematocrit as minimum markers. Post-cycle recovery timelines must explicitly account for depot duration on long-ester formulations — the clock starts from compound clearance, not last injection. These are not optional refinements to an otherwise complete protocol — they are the framework the compound’s pharmacology requires.
This article is published for educational and harm-reduction purposes only. Nandrolone and all anabolic compounds discussed here are controlled substances in most jurisdictions. Nothing in this guide constitutes medical advice, a recommendation to use any compound, or guidance on sourcing or legal compliance. Readers assume full responsibility for any decisions made on the basis of information presented here.
All content on MuscleScience.org is produced by contributors working under pseudonyms for editorial independence and personal privacy. Author photographs are stylized portraits, not real images of the writers. See our About page for full editorial and anonymity disclosure.
We do not sell. We do not supply. We educate.


