HDL, LDL & Triglycerides Explained
Reading your cholesterol panel
A lipid panel is one of the most important bloodwork tools for understanding cardiovascular context before deeper PED, TRT, hormone, or performance-health decisions. HDL, LDL, triglycerides, total cholesterol, and related markers help show how the body is handling blood fats, cardiovascular risk patterns, and long-term health pressure — and none of it is visible from the outside.
Lipid Panel Markers in Plain Language
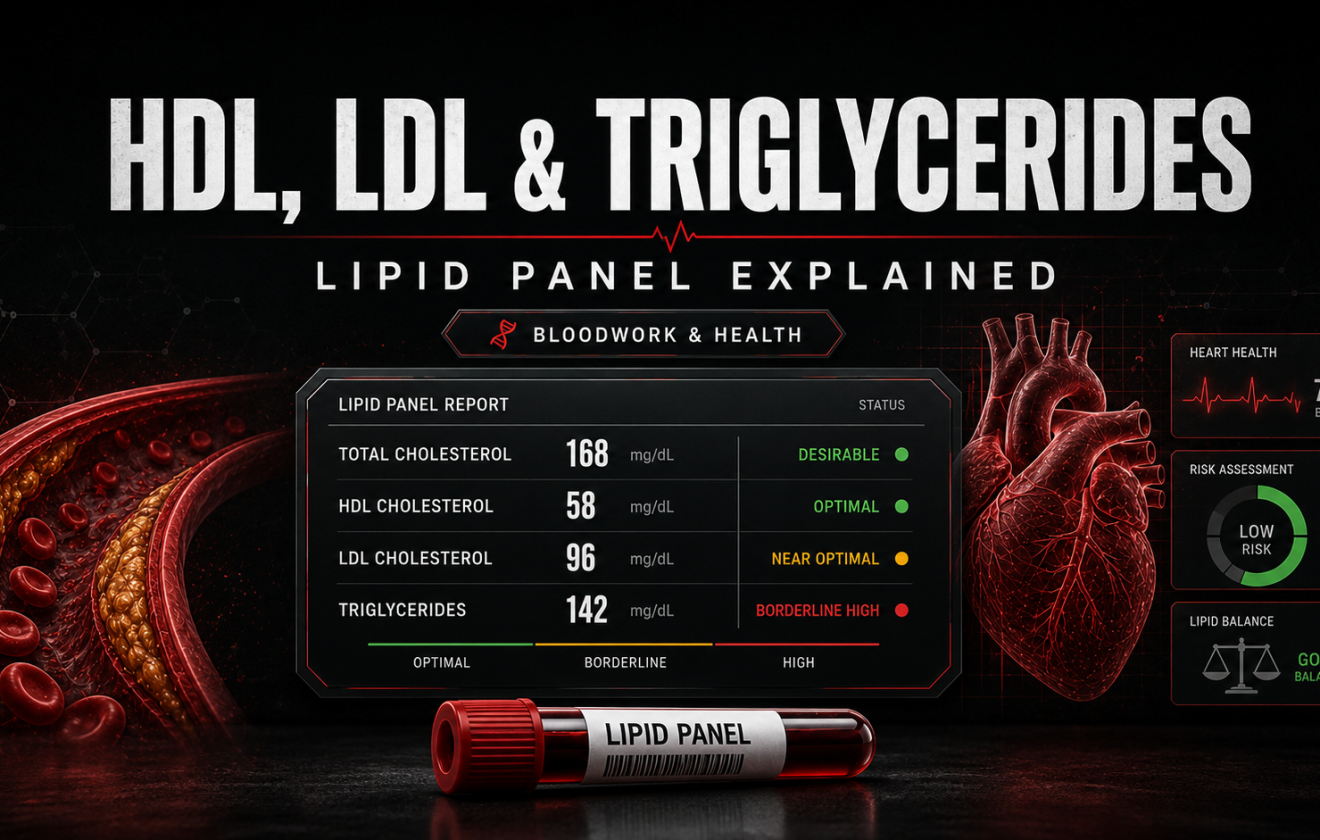
A lipid panel is a blood test that measures cholesterol and fat-related markers in the bloodstream. The standard markers include total cholesterol, LDL cholesterol, HDL cholesterol, and triglycerides. Some panels or clinicians also include non-HDL cholesterol, ApoB, or lipoprotein(a) when deeper cardiovascular risk context is needed.
In bodybuilding and PED discussions, lipid markers matter because cardiovascular risk is not something that announces itself through symptoms. A person can train hard, look athletic, maintain low body fat, and still carry unfavorable lipid patterns that affect arterial health over years — not weeks. The gym does not protect against a lab result.
The goal of a lipid panel is not to create anxiety over one number. The goal is to understand the pattern: what is LDL doing, what is HDL doing, where are triglycerides, and how do these markers fit with blood pressure, glucose, body composition, family history, smoking status, and PED exposure?
LDL is discussed because higher levels can contribute to arterial plaque buildup and cardiovascular risk over time.
HDL is involved in reverse cholesterol transport. It should be read as part of a full pattern, not a standalone safety score.
Triglycerides reflect blood fat levels and connect with diet, alcohol, insulin sensitivity, and broader metabolic health.
Contents
What This Lipid Panel Guide Covers
This guide explains HDL, LDL, triglycerides, total cholesterol, and non-HDL cholesterol — and why these markers matter in the context of performance health, PED education, TRT monitoring, and cardiovascular risk awareness. It is written for readers who want to understand bloodwork, not just collect numbers.
It does not tell a reader how to treat abnormal cholesterol, whether to start medication, or how to make personal medical decisions. Lipid interpretation depends on age, sex, family history, blood pressure, diabetes risk, smoking, medications, diet, body composition, and clinical history. One number on a panel does not tell the full story.
- Covered: HDL, LDL, triglycerides, total cholesterol, non-HDL cholesterol, ApoB context, fasting status, PED and TRT context, and common mistakes.
- Not covered: personal diagnosis, medication decisions, cycle design, drug protocols, or individualized cardiovascular treatment.
- Best use: read this after the Blood Tests Before Steroids guide and the Hematocrit and Hemoglobin article, then connect it with blood pressure, glucose, and hormone monitoring for the full picture.
What a Lipid Panel Usually Measures
A lipid panel gives a snapshot of several fat-related markers in the bloodstream. Most people recognize it as a cholesterol test, but calling it that undersells what it shows. The individual markers within a lipid panel tell different parts of the cardiovascular story — and the pattern across all of them is more informative than any single value.
Total cholesterol is the broadest number. LDL, HDL, and triglycerides provide the detail that makes total cholesterol interpretable. In many cases, non-HDL cholesterol adds another useful lens because it captures cholesterol carried by atherogenic particles that are not HDL — a view that can matter when LDL alone understates the risk picture.
Total Cholesterol
Total cholesterol is the sum of LDL, HDL, and a fraction of triglycerides. It can flag a general concern, but it is not enough by itself. Two people can have identical total cholesterol with very different LDL, HDL, and triglyceride profiles — and those differences matter clinically. Treating total cholesterol as the final word is one of the more common ways to misread a lipid panel.
LDL Cholesterol
LDL is the marker most associated with arterial plaque development and atherosclerotic cardiovascular risk. Higher LDL — especially over years — can contribute to plaque accumulation in arterial walls, affecting blood flow and increasing the risk of serious cardiovascular events. In performance culture, LDL can be underestimated because people associate visual fitness with internal health. That association is unreliable.
HDL Cholesterol
HDL is involved in reverse cholesterol transport — moving cholesterol back toward the liver for processing. Higher HDL is generally viewed as favorable. But HDL should not be used as a standalone safety signal. A high HDL number does not neutralize high LDL, high blood pressure, smoking, or family history. It shifts the context, not the conclusion.
Triglycerides
Triglycerides are a type of fat circulating in the blood. They rise with excess calories, high refined carbohydrate intake, alcohol use, poor insulin sensitivity, certain medications, genetics, and metabolic dysfunction. In a lipid panel, triglycerides connect cholesterol numbers with the broader picture of energy handling, metabolic health, and insulin function. High triglycerides combined with low HDL is a pattern that deserves particular attention.
Why the Lipid Panel Matters for PED and TRT Discussions
PED conversations tend to focus on visible or felt effects: strength, muscle size, recovery speed, water retention, libido, mood, and injection site issues. Lipids are invisible and produce no immediate symptoms. A person does not feel LDL rising or HDL dropping in real time — which is exactly what makes lipid monitoring important rather than optional.
Anabolic-androgenic steroid use is associated in medical literature with unfavorable lipid shifts in some users. The most consistently documented pattern is a significant drop in HDL — sometimes to very low levels — combined with rising LDL. Oral compounds, particularly those with a 17-alpha alkylated structure, tend to produce more dramatic lipid changes than injectable compounds, but injectable androgens are not without lipid effects. Compound choice, dose, duration of use, genetics, diet quality, body fat, and baseline health all influence the magnitude of change.
TRT is a different clinical context from unsupervised PED use, but lipid monitoring still belongs in the conversation. Someone on medically supervised testosterone therapy may have their lipids reviewed as part of standard cardiovascular risk management. Someone researching PEDs outside of medical care has no automatic safety net — which makes understanding lipid markers more important, not less. For the full monitoring picture in a TRT context, read TRT Bloodwork.
The concern is not any single lipid number. The concern is cumulative risk. If LDL is rising, HDL is falling, blood pressure is climbing, hematocrit is elevated, and triglycerides are worsening at the same time — the combined picture represents meaningfully higher cardiovascular risk than any marker would suggest in isolation. Read Blood Pressure Before Steroids for the full cardiovascular context alongside lipids.
How to Think About HDL Cholesterol
HDL is commonly described as protective because it is involved in moving cholesterol from tissues and arterial walls back toward the liver for processing. In basic terms, HDL is helping clear cholesterol from places where it can cause damage and return it to where it can be handled. That is why higher HDL has traditionally been associated with lower cardiovascular risk.
In PED discussions, low HDL is one of the patterns that consistently appears in harm-reduction conversations and medical literature. If HDL drops while LDL rises — a common direction with some anabolic-androgenic compounds — the overall lipid risk picture worsens on both ends simultaneously. That dual shift is more concerning than either marker changing alone.
HDL is not a static number. It can be influenced by genetics, diet quality, body composition, alcohol intake, smoking, exercise type and intensity, medications, hormone status, and anabolic steroid exposure. The most useful framing is not only “what is my HDL number?” but “what was my HDL before, what has changed since, and what may have caused the shift?”
Very high HDL also warrants interpretation rather than automatic celebration. Extremely elevated HDL in some contexts may reflect other underlying issues rather than exceptional protection. As with most bloodwork markers, the useful data is in the pattern and trend, not in a single value compared against a reference range.
How to Think About LDL Cholesterol
LDL is one of the primary markers used in cardiovascular risk assessment because it is the main carrier of cholesterol to tissues and arterial walls. When LDL is elevated chronically, the risk of plaque accumulation — atherosclerosis — rises, especially in the presence of other risk factors such as high blood pressure, smoking, inflammation, diabetes risk, or family history.
In bodybuilding culture, LDL can be systematically underestimated because people associate visible leanness, athletic performance, and regular training with cardiovascular health. That association breaks down quickly when lipids, blood pressure, and bloodwork are actually reviewed. Lean mass and strength do not erase lipid risk — they simply do not correlate with it as strongly as appearance suggests.
LDL should be read in the context of the full lipid panel. For some individuals — particularly those with strong family history, repeatedly abnormal labs, or advanced PED exposure — ApoB or non-HDL cholesterol may offer additional precision about the number of atherogenic particles circulating, which can sometimes tell a different story than LDL alone. These are conversations to have with a qualified healthcare professional, not conclusions to draw from a forum post.
How to Think About Triglycerides
Triglycerides are strongly connected to energy balance, dietary habits, and metabolic context. They tend to rise with caloric surplus, high refined carbohydrate or sugar intake, alcohol use, poor insulin sensitivity, sedentary patterns, certain medications, genetics, and metabolic conditions. Because of their sensitivity to diet and lifestyle, triglycerides should ideally be measured fasting for the most reliable comparison across tests.
For bodybuilders, triglycerides can shift noticeably during bulking phases — more calories, more carbohydrates, and sometimes more alcohol or poor food choices. A person who looks muscular and trains consistently can still have elevated triglycerides if the underlying dietary and metabolic context is unfavorable.
Triglycerides matter in the lipid panel because they interact with the full picture. High triglycerides combined with low HDL is one of the patterns associated with insulin resistance and metabolic syndrome. High triglycerides combined with high LDL and elevated blood pressure stacks the risk context further. No single elevated triglyceride reading is a verdict — but a persistent pattern across multiple tests is worth taking seriously.
Where Does a Reading Fall?
Drag each slider to see the zone for an LDL, HDL, or triglyceride value. Note that for HDL, higher is generally better, so the colours are reversed. Bands are illustrative adult guides, not diagnostic — labs and clinical targets vary by individual risk.
Illustrative adult ranges only — not diagnostic and not a target for any individual. HDL thresholds differ by sex (below about 50 mg/dL is considered low in women vs about 40 in men). Interpretation belongs to a clinician who weighs your overall cardiovascular risk.
Non-HDL Cholesterol, ApoB, and Lipoprotein(a)
A standard lipid panel gives useful information, but it is not the complete picture for every person. Some clinicians use additional markers when they need a more precise view of cardiovascular risk — particularly when standard lipid numbers look borderline, when family history is significant, or when PED exposure has been part of the clinical context.
Non-HDL cholesterol is calculated by subtracting HDL from total cholesterol. It captures cholesterol carried by all atherogenic particles — not just LDL — which makes it a broader measure of cardiovascular particle burden. For some people, non-HDL cholesterol tells a more complete story than LDL alone.
ApoB measures the total number of atherogenic lipoprotein particles directly. Because each LDL, VLDL, and IDL particle carries one ApoB protein, ApoB gives insight into particle count rather than just particle cholesterol content. In people where LDL underestimates risk — such as those with elevated triglycerides or metabolic dysfunction — ApoB may be a more accurate cardiovascular risk marker.
Lipoprotein(a), or Lp(a), is largely genetically determined and not significantly modified by lifestyle. It can matter in people with family history of premature cardiovascular disease or unexplained risk that does not fit the standard lipid pattern. Not everyone needs Lp(a) testing, but it can be part of a more thorough cardiovascular risk assessment when standard panels do not fully explain the picture.
Fasting, Timing, and Repeat Testing
Lipid panels can be done fasting or non-fasting depending on the clinical context. Triglycerides are the marker most affected by recent food intake — a meal heavy in fat or carbohydrates can significantly raise triglyceride levels for hours afterward. For this reason, fasting lipid panels are generally preferred when comparing results across different tests or tracking trends over time.
Timing relative to lifestyle variables also matters. A lipid panel taken during a caloric surplus bulk, after a heavy alcohol weekend, during illness, after poor sleep, or in the middle of significant PED exposure reflects those conditions — not a stable baseline. That does not make the result useless, but it changes how it should be weighted against other tests taken under more controlled conditions.
Repeat testing over time is more valuable than any single panel. One result is a data point. Several results under similar conditions — with clear notes on fasting status, recent diet, alcohol, illness, training stress, bodyweight, and hormone exposure — form a pattern that can actually inform decisions.
How the Lipid Panel Connects With the Rest of Bloodwork
The lipid panel is most useful when it is not read in isolation. Lipids interact with other systems in the body, and the risk picture changes substantially depending on what else is happening in the bloodwork.
Blood pressure and lipids belong in the same cardiovascular conversation. Elevated LDL combined with high blood pressure is more concerning than either marker alone — blood pressure drives mechanical stress on arterial walls while LDL contributes to plaque formation in those same walls. For the full blood pressure context, read Blood Pressure Before Steroids.
Hematocrit and hemoglobin interact with the cardiovascular picture too. Elevated hematocrit increases blood viscosity — making the blood thicker and harder to move — which adds mechanical load on the same vascular system that elevated LDL is affecting. Read Hematocrit and Hemoglobin CBC Markers for that context.
Liver markers are relevant because the liver is central to cholesterol metabolism. It produces, processes, and clears cholesterol — and liver stress from oral anabolic compounds can affect both liver marker values and lipid handling at the same time. Read Liver Markers: AST, ALT & GGT to understand how those markers connect. Kidney function, covered in the Kidney Markers: Creatinine, eGFR & BUN guide, adds another layer to the cardiovascular risk picture when pressure or metabolic stress is involved.
Where People Usually Get Lipid Panels Wrong
The first mistake is reading only total cholesterol. Total cholesterol can conceal very different underlying patterns. A person with high HDL and modest LDL has a fundamentally different risk picture from someone with low HDL, high LDL, and elevated triglycerides — even when total cholesterol is identical on both panels.
The second mistake is assuming visible fitness provides protection. Training improves many cardiovascular markers, but it does not guarantee a clean lipid panel — especially when PED exposure, genetics, diet quality, or high blood pressure are also in the picture. Leanness and strength are useful traits, but they are not a proxy for lipid health.
The third mistake is ignoring baseline. If someone only checks lipids after months of changes, they cannot know what was already abnormal before, what shifted recently, or what the trajectory has been. A baseline drawn before any compound or major lifestyle change is the only true reference point for everything that follows.
- Only checking total cholesterol: LDL, HDL, triglycerides, and non-HDL cholesterol usually provide more meaningful cardiovascular context than the headline number alone.
- Ignoring HDL drops: a significant HDL decline matters, especially when LDL is rising at the same time — the dual shift worsens the risk picture on both ends simultaneously.
- Forgetting blood pressure: lipid markers and blood pressure belong in the same cardiovascular risk conversation and should always be reviewed together.
- Assuming “fit” means protected: visible muscularity and gym performance do not guarantee low cardiovascular risk or favorable lipid panels.
- Self-treating abnormal labs: persistently abnormal lipid markers should be reviewed with qualified medical context before any management decisions are made.
Frequently Asked Questions
Why do steroids lower HDL and raise LDL?
How fast do lipids change on cycle?
Is a high LDL from muscle or diet?
What is ApoB and should I test it?
Should I fast before a lipid panel?
How does this fit the rest of my bloodwork?
How to Use a Lipid Panel Without Guesswork
A lipid panel is a context tool, not a verdict. It helps show whether the cardiovascular side of the bloodwork picture is trending in a favorable or unfavorable direction — and in a PED or TRT context, that direction matters far more than any single gym session or visual impression of health.
The useful questions are: what was the baseline before any change, what shifted since, what else changed at the same time, and what does a qualified healthcare professional think about the overall pattern? One abnormal result is a data point. A repeated direction across multiple tests under similar conditions is a signal worth acting on clinically.
Continue with the Bloodwork & Health hub for all related marker guides. Review the full TRT Bloodwork article to understand how lipid monitoring fits into ongoing hormone therapy follow-up. Explore the TRT & Hormones section for the endocrine context. Use the Start Here page to find the right reading path.
Medical Resources and Reference Reading
The following sources provide additional clinical background on lipid panel markers, cardiovascular risk, and the effects of anabolic-androgenic steroids on lipid profiles for readers who want to go deeper into the evidence base.
Final Educational Note
Muscle Science is an educational resource. This article is for general information only and does not replace medical advice, diagnosis, treatment, or care from a qualified healthcare professional.


