How Long Recovery Can Take After a Steroid Cycle
PCT Recovery Timeline: How Long It Can Take After a Steroid Cycle
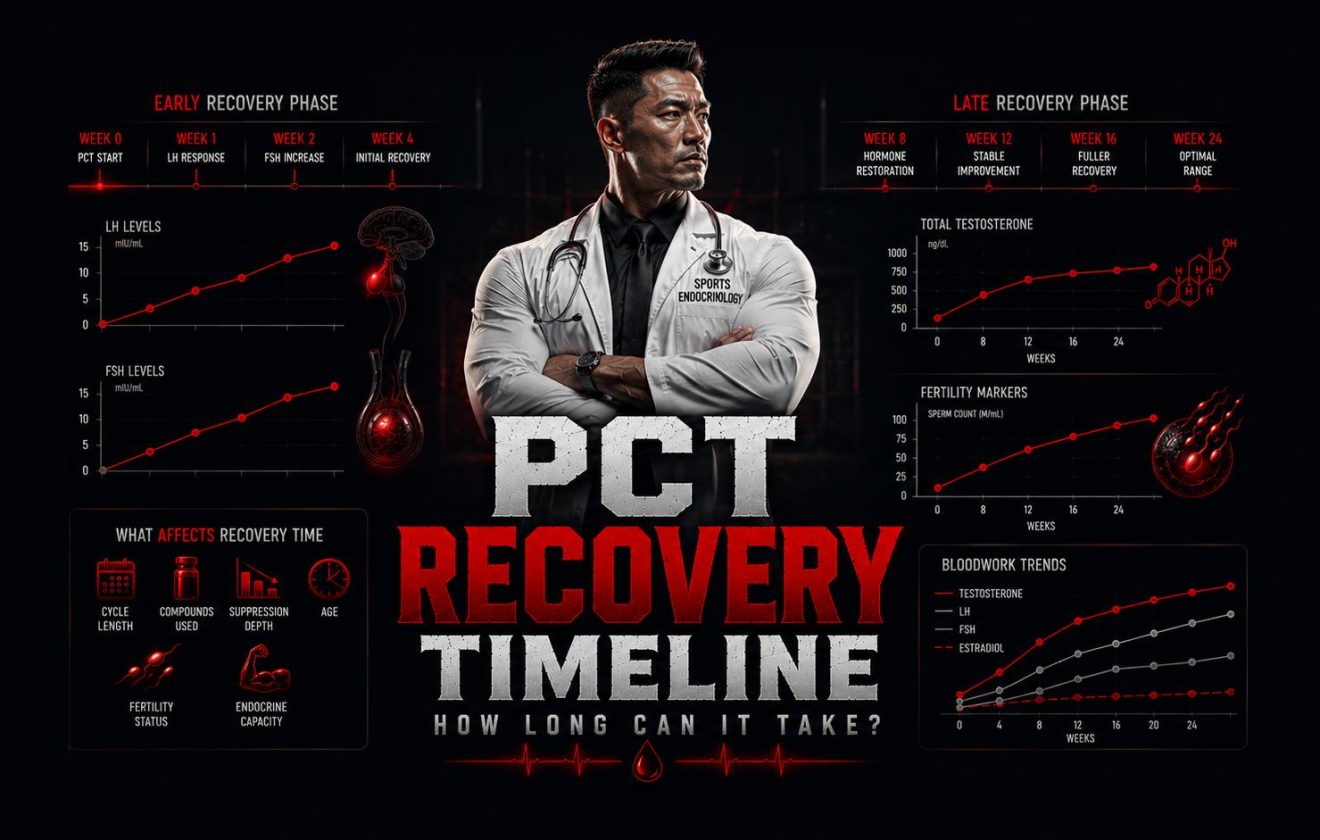
The PCT recovery timeline is not a single fixed endpoint — it is a sequence of biological milestones that unfold at different rates and are governed by separate hormonal signals. Understanding how the PCT recovery timeline works, what it actually measures, and which variables control it is the foundation for any structured recovery after a steroid cycle.
PCT Recovery Timeline: Three Stages, Three Timescales
The PCT recovery timeline unfolds in a defined sequence — not all at once. Each stage is governed by a different hormonal signal and restores at its own rate. Most errors in PCT happen because users treat all three stages as a single event.
Stage 1 — Gonadotropins
LH and FSH are the first markers to recover in the PCT recovery timeline. PCT drugs act here — at the hypothalamic level — to restart GnRH pulsatility and drive pituitary output. Without LH and FSH, nothing downstream can follow.
Stage 2 — Testosterone
Once LH signals the Leydig cells, endogenous testosterone synthesis resumes. This is the most commonly tracked marker, but it is the second stage of the PCT recovery timeline — not the first, and not the last. Normalization typically lags 6–22 weeks behind PCT initiation depending on cycle profile.
Stage 3 — Spermatogenesis
The slowest stage of the PCT recovery timeline. Sperm production lags behind testosterone recovery by months. A complete spermatogenic cycle takes ~74 days, and this stage is only confirmed by semen analysis — not by a hormone panel.
What This Guide Covers
Covered in This Guide
- What the PCT recovery timeline actually measures — the three biological endpoints
- How the HPTA controls the recovery cascade from hypothalamus to testes
- Six variables that determine your personal PCT recovery timeline
- Typical recovery ranges by cycle intensity
- Five mistakes that consistently extend the PCT recovery timeline
- How to confirm recovery through bloodwork
Not Covered Here
- Specific PCT drug protocols (tamoxifen / clomiphene dosing)
- When to start PCT by compound — see the dedicated guide
- TRT as an alternative to natural recovery
- Fertility treatment beyond the scope of steroid suppression
- Bloodwork interpretation — covered in the PCT bloodwork guide
Recommended reading order. This article covers the PCT recovery timeline as a biological process. For the suppression mechanism that precedes it, see Why Steroids Cause Testosterone Suppression. For the full recovery sequence step by step, see How Hormonal Recovery Works After Steroids.
What the PCT Recovery Timeline Actually Measures
The PCT recovery timeline is not a single variable. It is a layered biological process with three distinct endpoints, each driven by a different hormonal signal and each restoring on its own schedule. Most users track the PCT recovery timeline by how they feel — energy is back, libido has returned, mood has stabilized. This is the wrong endpoint. Subjective improvement precedes bloodwork recovery by weeks, and in some cases by months.
The only valid measure of a complete PCT recovery timeline is a confirmed hormone panel showing LH, FSH, and total testosterone returned to pre-cycle or age-appropriate baseline — and a semen analysis for anyone with fertility goals. The four points below define what a complete PCT recovery timeline measures as a biological process.
LH & FSH Restoration
The first stage of the PCT recovery timeline. Luteinizing hormone (LH) and follicle-stimulating hormone (FSH) are suppressed by exogenous androgens via negative feedback on the hypothalamus and pituitary. PCT drugs — primarily tamoxifen and clomiphene — block estrogen receptors at the hypothalamic level, releasing the brake on GnRH pulse generation and driving the pituitary to secrete LH and FSH again. Until gonadotropins are actively signaling the testes, the remainder of the PCT recovery timeline cannot proceed.
Total Testosterone Normalization
Once LH signals the Leydig cells, endogenous testosterone synthesis resumes. The speed at which total testosterone returns to baseline depends on Leydig cell responsiveness — determined by how long they were inactive, which compounds were used, and individual genetic sensitivity. For a testosterone-only cycle this point in the PCT recovery timeline is typically reached in 8–14 weeks. For heavy 19-nor cycles, it can take 4–7 months. This is the most commonly tested marker, but it remains only the second of three PCT recovery timeline endpoints.
Spermatogenesis Recovery
The third and slowest endpoint of the PCT recovery timeline. Sperm production is governed primarily by FSH acting on Sertoli cells, combined with high intratesticular testosterone. Because a complete spermatogenic cycle takes approximately 74 days plus transit time, even after LH and testosterone have fully normalized, sperm count may remain severely impaired for months. A user can have completely normal hormone bloodwork and still be functionally infertile. This stage extends the PCT recovery timeline well beyond the hormonal window for anyone with fertility goals.
Bloodwork as the Only Confirmation
None of the three PCT recovery timeline endpoints can be confirmed subjectively. Energy and libido can recover while testosterone remains below baseline. Testosterone can normalize while sperm count remains critically low. The only way to know where you are in the PCT recovery timeline is through a hormone panel at defined intervals. Bloodwork before and after PCT defines what recovery means as a measured number, not as a feeling.
On timing: When you initiate PCT relative to your last injection is a separate variable that affects the entire PCT recovery timeline. Starting too early wastes the protocol window. Starting too late extends unassisted suppression. See When to Start PCT After a Steroid Cycle for the compound-specific clearance framework.
How the HPTA Controls the PCT Recovery Timeline
The PCT recovery timeline is governed entirely by the hypothalamic-pituitary-testicular (HPTA) axis — the hormonal feedback loop that regulates endogenous testosterone and sperm production. When exogenous androgens are introduced, this loop shuts down: the hypothalamus and pituitary reduce GnRH, LH, and FSH output because androgens are already present. The testes go functionally dormant. The PCT recovery timeline is the process of restarting that system — and it does not happen instantly or uniformly.
The speed of the PCT recovery timeline depends on how deeply each component of the HPTA was suppressed and for how long. A lightly suppressed axis with residual LH and FSH activity throughout the cycle has a shorter path to recovery than one that was fully shut down for 20 weeks. The compound used determines suppression depth: testosterone-based cycles suppress via androgen and estrogen feedback; 19-nortestosterone compounds add a progestogenic mechanism that makes the PCT recovery timeline significantly longer and less predictable.
The three components below define the HPTA recovery cascade. Recovery does not begin in the testes. It begins in the brain — and the PCT recovery timeline is only as fast as the slowest link in this chain.
Hypothalamus
The first component to recover in the PCT recovery timeline. The hypothalamus resumes pulsatile GnRH secretion once the negative feedback from exogenous androgens is removed. PCT drugs accelerate this by blocking estrogen receptors at the hypothalamic level, releasing the brake on GnRH pulses. Without restored GnRH pulsatility, the pituitary cannot resume LH and FSH secretion and the downstream cascade cannot begin.
Pituitary Gland
Responds to restored GnRH pulses by secreting LH and FSH. LH drives Leydig cell testosterone synthesis; FSH drives Sertoli cell support of spermatogenesis. The pituitary’s response amplitude and timing directly determine the pace of the PCT recovery timeline from this point forward. Tamoxifen and clomiphene both enhance pituitary sensitivity to GnRH by blocking the estrogenic suppression at the receptor level.
Testes
The final and slowest component of the PCT recovery timeline. Leydig cells respond to LH by resuming testosterone synthesis, but require time to restore full secretory capacity after a period of inactivity — particularly after long or heavy cycles. Sertoli cells, responding to FSH, must restart the full 74-day spermatogenic cycle. Testicular recovery is the rate-limiting step in the PCT recovery timeline for most users, especially those with fertility goals.
Poor responders exist. Research documents that approximately 20% of users who cease anabolic steroid use do not achieve satisfactory recovery on a standard PCT recovery timeline. Age, prior HPTA function, and individual Leydig cell responsiveness all contribute. See How Hormonal Recovery Works After Steroids for the full biological sequence.
6 Factors That Determine Your PCT Recovery Timeline
The PCT recovery timeline is not uniform. The range between a fast recovery and a prolonged one is not random — it is driven by specific, identifiable variables that interact with each other. Understanding which factors are working for or against you is what allows the PCT recovery timeline to be planned and monitored rather than simply waited out.
Two users running the same PCT protocol can have dramatically different outcomes. The six variables below explain why. Each one affects a different part of the PCT recovery timeline — suppression depth, axis responsiveness, or the endpoint being tracked.
Compound Type
This is the single most influential variable in the PCT recovery timeline. Testosterone-only cycles suppress the HPTA, but the axis responds relatively well once the compound clears. Cycles involving 19-nortestosterone compounds — nandrolone, trenbolone — suppress LH and FSH far more aggressively and for longer. The progestogenic activity of 19-nor compounds compounds their suppressive effect, and recovery from a nandrolone-based cycle routinely extends the PCT recovery timeline 2–3 times longer than a comparable testosterone-only cycle.
Cycle Length
The longer the HPTA remains suppressed, the more the glands — particularly the testes — adapt to an inactive state. An 8-week cycle leaves the Leydig cells dormant for a shorter window than a 20-week cycle. Duration is cumulative: each additional week of suppression adds to the baseline that the PCT recovery timeline has to overcome. Short cycles of 8–10 weeks on testosterone alone typically complete the PCT recovery timeline in 10–16 weeks. Cycles of 16–20 weeks, particularly with multiple compounds, extend that window significantly.
Suppression Depth
Not all suppression is equal. Some compounds nearly abolish LH and FSH output within weeks. Others produce partial suppression where gonadotropins remain detectable throughout the cycle. The depth of suppression — measured by how low LH, FSH, and endogenous testosterone dropped at the nadir — directly predicts how much ground the PCT recovery timeline has to cover. Users who maintained some residual HPTA activity during a cycle typically recover faster than those with complete shutdown.
Age
Younger men with robust baseline HPTA function generally move through the PCT recovery timeline faster. The Leydig cells of a 22-year-old respond more aggressively to restored LH signaling than those of a 42-year-old, whose baseline testosterone production was already declining. Age also affects baseline sperm parameters — older men may achieve hormonal markers on schedule while still experiencing delayed spermatogenesis recovery.
Fertility Goals
The endpoint being tracked determines how long the PCT recovery timeline extends. If the goal is hormonal recovery — LH, FSH, and total testosterone back to baseline — the timeline is measured in weeks to months. If the goal is fertility — restoring sperm count, motility, and morphology — the PCT recovery timeline extends dramatically. Spermatogenesis recovery lags behind hormonal recovery by months. Normal bloodwork and adequate sperm production are different endpoints that require separate evaluation and separate confirmation methods.
Individual HPTA Responsiveness
Genetic and constitutional variation is real and it affects the PCT recovery timeline in ways that cannot be predicted in advance. Published research consistently shows that approximately 20% of users who cease anabolic steroid use do not achieve satisfactory hormonal recovery even after several months. Some individuals have inherently slower Leydig cell response or pre-existing subclinical hypogonadism masked by exogenous androgens. This is why bloodwork at defined intervals is the only reliable method for confirming where the PCT recovery timeline actually stands.
Timing the PCT start correctly matters. When you initiate PCT relative to your last injection is a variable that affects the entire PCT recovery timeline. Starting too early wastes the protocol window on still-active compound. Starting too late extends unassisted suppression. See When to Start PCT After a Steroid Cycle for the compound-by-compound clearance framework.
PCT Recovery Timeline Ranges by Cycle Intensity
The following ranges reflect the general pattern seen in clinical observations and published literature. They represent what the PCT recovery timeline looks like across different cycle profiles — not a personal prediction. The six factors above interact to shift any individual’s PCT recovery timeline earlier or later than the ranges shown. The only way to know where you stand is through bloodwork at defined intervals.
These ranges cover the hormonal PCT recovery timeline only. Spermatogenesis recovery extends beyond every range shown here. Users with fertility goals should consult semen analysis data, not hormone panels, as the relevant endpoint.
| Cycle Profile | LH & FSH Recovery | Total Testosterone | Sperm Count |
|---|---|---|---|
| Mild — testosterone only, 8–10 weeks | 4–6 weeks into PCT | 8–14 weeks | 3–6 months |
| Moderate — testosterone + oral compound, 12–16 weeks | 6–10 weeks into PCT | 14–22 weeks | 6–12 months |
| Heavy — 19-nor based (nandrolone/trenbolone), 16–20+ weeks | 10–18 weeks into PCT | 4–7 months | 12–18+ months |
| Poor responders (~20% of users, any profile) | Delayed or incomplete | May not normalize without intervention | Unpredictable |
Ranges derived from published clinical data on HPG axis recovery and spermatogenesis restoration following anabolic steroid cessation. The PCT recovery timeline varies significantly between individuals. Bloodwork at 4, 8, and 12 weeks post-PCT provides the actual data for your specific recovery.
The 20% rule. Research documents that roughly 1 in 5 users will not achieve satisfactory hormone recovery on a standard PCT recovery timeline, regardless of cycle intensity. This is a documented finding in prospective observational studies, not an anecdotal outlier. Age, pre-existing HPTA function, and genetic responsiveness all contribute. Follow-up bloodwork is the only way to identify poor responders before the situation becomes clinical hypogonadism.
5 Mistakes That Extend the PCT Recovery Timeline
Most delays in PCT recovery are not biological inevitabilities — they are the result of avoidable decisions made before, during, or after the cycle ends. These are the five patterns that consistently extend the PCT recovery timeline beyond what the underlying suppression alone would have required.
- Mistake 1
Using Subjective Feeling as the Recovery Marker
“I feel normal again” is not a valid endpoint for the PCT recovery timeline. Mood, libido, and energy can improve well before total testosterone, LH, and FSH normalize. This is because partial testicular function and adrenal androgen production can create a subjective sense of wellbeing while the HPTA is still measurably suppressed. Men who end PCT or start a new cycle based on how they feel — rather than what their bloodwork shows — are making decisions without data. Post-PCT bloodwork is the only valid confirmation of where the PCT recovery timeline actually stands.
- Mistake 2
Treating Hormone Recovery as Fertility Recovery
Normal testosterone on bloodwork does not mean normal sperm production. These are separate biological processes driven by different hormonal signals — LH governs testosterone synthesis, FSH governs spermatogenesis. A man can have normal LH, FSH, and testosterone and still have severely impaired sperm count, because spermatogenesis lags behind steroidogenesis by months. Anyone planning to father children within 12–18 months of a cycle needs semen analysis, not just a hormone panel. See the full picture in Fertility and Suppression on Steroids.
- Mistake 3
Starting the Next Cycle Before Confirmed Recovery
Running back-to-back cycles without allowing full HPTA restoration is cumulative suppression that compounds with each cycle. Every cycle that starts before the PCT recovery timeline is complete adds to the total suppression burden and compresses the axis’s capacity to restart independently. Men who run multiple cycles with short gaps frequently discover that the PCT recovery timeline has become increasingly prolonged — or that natural recovery is no longer possible without medical intervention. The PCT recovery timeline exists for a reason. Cutting it short permanently compounds the problem.
- Mistake 4
Cutting PCT Short Because Early Symptoms Improved
PCT drugs like tamoxifen and clomiphene stimulate LH and FSH, which drives early testosterone recovery. This produces noticeable improvement in energy and libido within the first two to three weeks — which some users interpret as the end of the PCT recovery timeline. The early improvement reflects the pharmacological action of the drug, not the restored autonomous function of the HPTA. Stopping too soon removes the stimulus before the axis has learned to function independently, and the hormones drop again, resetting the PCT recovery timeline.
- Mistake 5
Not Running Bloodwork Before Starting PCT
Without a baseline suppression measurement — taken at the end of cycle washout, before PCT begins — there is no defined start point for the PCT recovery timeline and no target to recover to. Knowing your suppressed LH, FSH, and total testosterone allows you to set a concrete endpoint and verify when you have genuinely reached it. Without this data, the PCT recovery timeline has no verifiable finish line. Bloodwork before and after PCT converts the PCT recovery timeline from a guessing exercise into a measurable, confirmable process.
- Blood Tests Before Steroids: 7 Markers to Check — the 7-marker baseline panel to run before starting
Research Cited in This Article
- Solanki P, Eu B, Smith J, Allan C, Lee K. Physical, psychological and biochemical recovery from anabolic steroid-induced hypogonadism: a scoping review. Endocrine Connections. 2023;12(12):e230358. PMID 37855241
- Grant B, Pradeep A, Minhas S, Dhillo WS, Quinton R, Jayasena CN. Survey of endocrinologists managing recovery from anabolic androgenic steroid induced hypogonadism. Reproduction and Fertility. 2023;4(1):e220097. PMID 36757334
- Lykhonosov MP, Babenko AY, Korneyev IA, et al. Peculiarity of recovery of the hypothalamic-pituitary-gonadal axis in men after using androgenic anabolic steroids. Problems of Endocrinology. 2020. PMID 33351319
- McBride JA, Coward RM. Recovery of spermatogenesis following testosterone replacement therapy or anabolic-androgenic steroid use. Asian Journal of Andrology. 2016;18(3):373–380. PMID 26908067
- Desai A, Yassin M, Cayetano A, Tharakan T, Jayasena CN, Minhas S. Understanding and managing the suppression of spermatogenesis caused by testosterone replacement therapy and anabolic-androgenic steroids. Therapeutic Advances in Urology. 2022;14:17562872221105017. PMID 35783920
- Neto JOV, da Silva CA, Lima AB, Caminha JSR, Pinto DV, Alves FR, Araújo JS, Daher EF. Disorder of hypothalamic-pituitary-gonadal axis induced by abusing of anabolic-androgenic steroids for short time: a case report. Andrologia. 2018;50(10):e13107. PMID 30039560
The PCT Recovery Timeline Is Measurable — Treat It That Way
The PCT recovery timeline unfolds in layers — gonadotropins first, testosterone second, spermatogenesis last — each on its own timescale, each influenced by the specifics of the compounds used, the duration of suppression, and how the individual HPTA responds. Understanding that the PCT recovery timeline is a sequence of distinct endpoints, not a single event, is what separates a structured recovery from one based on assumption.
The six variables covered in this article — compound type, cycle length, suppression depth, age, fertility goals, and individual HPTA responsiveness — determine the personal PCT recovery timeline. None of them can be bypassed. What can be controlled is the quality of the protocol and the discipline to confirm outcomes with bloodwork rather than subjective assessment. Skipping that confirmation step is how a temporary suppression becomes a permanent one.
Roughly 1 in 5 users will not complete the PCT recovery timeline satisfactorily on a standard protocol. That finding is not alarming if recovery is monitored. It becomes a problem when the PCT recovery timeline is declared complete based on how someone feels — and the next cycle begins before the axis has genuinely restored. That pattern, repeated, converts suppression into a clinical condition that requires medical management.
The articles below cover the full context around the PCT recovery timeline — from the suppression mechanism to bloodwork interpretation to fertility impact. Use them to build a complete, evidence-based picture before, during, and after the PCT window.
- What Is Post-Cycle Therapy — complete overview of PCT purpose, drugs, and structure
- Why Steroids Cause Testosterone Suppression — the HPTA feedback mechanism explained
- How Hormonal Recovery Works After Steroids — the biological sequence from shutdown to restart
- When to Start PCT After a Steroid Cycle — compound-by-compound clearance timing
- Bloodwork Before and After PCT — what to test and how to interpret recovery markers
- Fertility and Suppression on Steroids — why sperm recovery follows a different timeline than testosterone
- Total vs Free Testosterone — understanding your testosterone bloodwork results
- TRT Bloodwork — hormone panel reference ranges and what they mean
- PCT Hub — full index of post-cycle therapy articles on MuscleScience.org
- Bloodwork & Health Hub — all bloodwork and monitoring guides in one place
- Start Here — the recommended reading sequence for MuscleScience.org
For Educational Purposes Only
This article discusses the PCT recovery timeline and hormonal suppression for educational and harm-reduction purposes. It does not constitute medical advice and is not a substitute for consultation with a qualified physician or endocrinologist. The information provided reflects published research and is intended to support informed decision-making, not to encourage or facilitate the use of controlled substances.
MuscleScience.org does not sell any compounds, medications, or supplements. All author names are pseudonyms. Author photographs are stylized portraits, not images of real individuals. See our About page and Disclaimer for full disclosure on editorial policy and anonymity.


