What Are Anabolic Steroids?
What Are Anabolic Steroids?
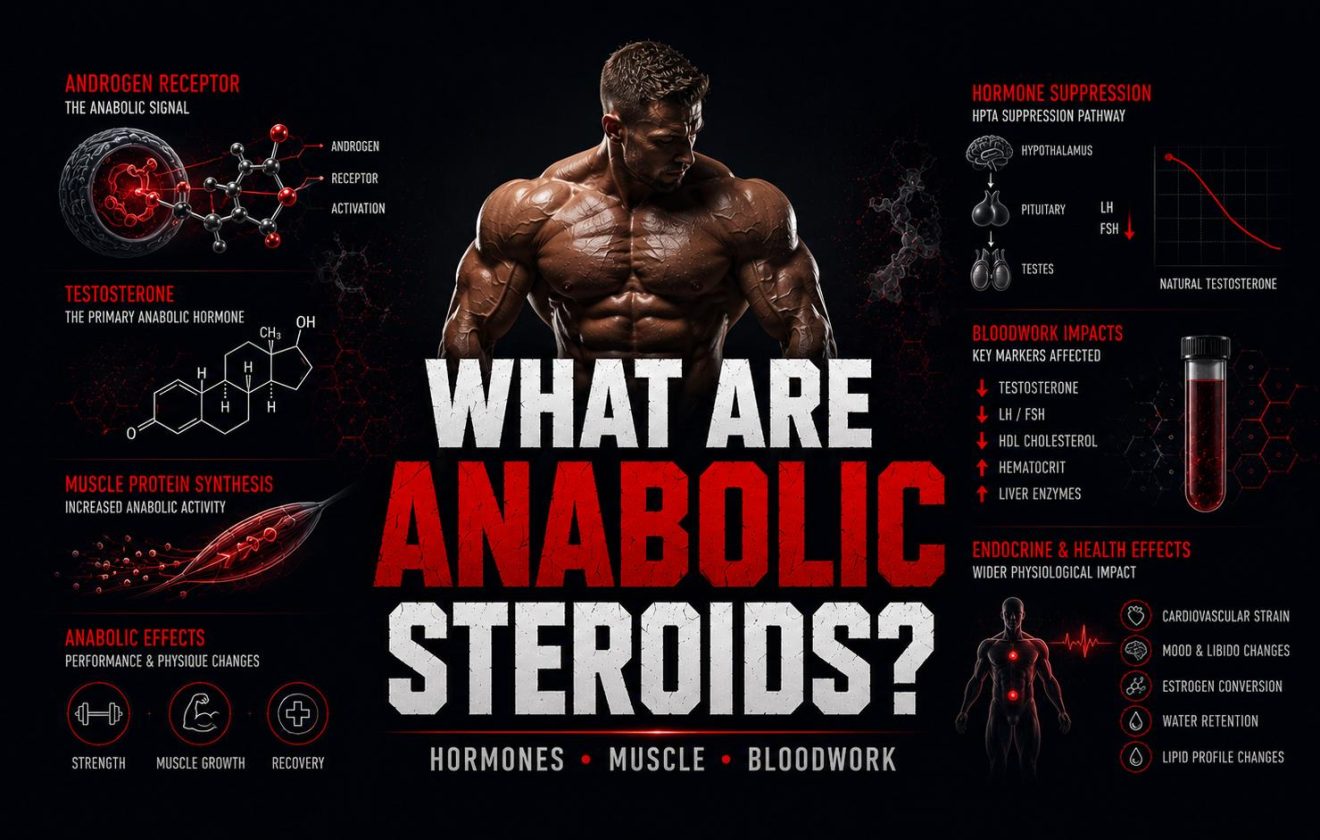
Anabolic steroids are synthetic derivatives of testosterone that bind to androgen receptors in muscle, bone, and connective tissue. Once bound, they activate gene expression linked to protein synthesis, nitrogen retention, and red blood cell production — the core mechanisms behind their performance effects. Understanding what anabolic steroids are, how they interact with the endocrine system, and what they do to bloodwork markers is the starting point of any evidence-based harm-reduction approach.
This guide covers the biology, the classification, the physiological effects, the hormonal consequences, and the bloodwork context that every person researching anabolic steroids needs before going further.
What Anabolic Steroids Are — Three Core Points
Definition
Anabolic steroids are synthetic testosterone derivatives engineered to replicate or amplify androgenic and anabolic signaling in target tissues throughout the body.
Mechanism
They bind to androgen receptors, translocate into the cell nucleus, and alter gene transcription — increasing muscle protein synthesis and reducing catabolic breakdown.
Bloodwork Impact
Anabolic steroids affect testosterone, LH, FSH, estradiol, HDL, hematocrit, liver enzymes, and kidney markers — baseline monitoring is mandatory for any harm-reduction framework.
What This Guide Covers
Covered in This Article
- Definition of anabolic steroids and AAS
- Androgen receptor mechanism
- Anabolic vs androgenic effects
- 6 key physiological effects
- Hormonal suppression and HPTA
- Bloodwork markers affected
- 5 common first-research mistakes
Not Covered Here
- Specific compound profiles
- Cycle dosing or scheduling
- PCT protocols in detail
- Vendor information
- Legal sourcing or purchasing
- Medical treatment or prescriptions
For compound-specific education, see the Steroids hub. For bloodwork context, see Bloodwork & Health. For post-cycle context, see PCT.
What Are Anabolic Steroids — Full Definition
Anabolic steroids — formally known as anabolic-androgenic steroids (AAS) — are synthetic compounds derived from testosterone. The term “anabolic” refers to tissue-building effects: muscle growth, nitrogen retention, increased red blood cell production. The term “androgenic” refers to masculinizing effects: facial hair development, voice deepening, oily skin, and changes in libido and aggression. Every anabolic steroid carries both properties to varying degrees. No compound is purely anabolic with zero androgenic activity — the ratio shifts, but both axes are always present.
The testosterone molecule has been chemically modified hundreds of times since the 1930s to produce compounds with altered anabolic-to-androgenic ratios, different half-lives, different oral or injectable bioavailability, and different metabolic pathways. This is why the category “anabolic steroids” includes dozens of distinct compounds — testosterone itself, nandrolone, stanozolol, oxandrolone, trenbolone, and many others — each with a distinct pharmacological profile and a distinct risk pattern.
Anabolic Steroids vs Corticosteroids
Corticosteroids — prednisone, hydrocortisone, dexamethasone — are a categorically different class of steroid hormone. They are derived from cortisol, not testosterone, and are primarily anti-inflammatory and immunosuppressive agents. When physicians say “steroids,” they almost always mean corticosteroids. When the performance and harm-reduction community says “anabolic steroids” or “AAS,” they mean testosterone-derived compounds that act on muscle, hormones, and androgenic signaling. These two classes share a naming convention but are mechanistically unrelated.
Legal Classification of Anabolic Steroids
In the United States, anabolic steroids are classified as Schedule III controlled substances under the Controlled Substances Act. In the United Kingdom, they are Class C substances under the Misuse of Drugs Act. Legal status varies significantly by country — some permit possession for personal use, others require a valid prescription, others prohibit all non-medical use entirely. This guide does not advise on legal compliance. That is entirely the reader’s responsibility.
How Anabolic Steroids Work — Androgen Receptor Activation
The primary mechanism of anabolic steroids is androgen receptor (AR) binding. Androgen receptors are intracellular proteins found in muscle cells, bone, prostate, skin, hair follicles, liver, and the central nervous system. When testosterone or a synthetic anabolic steroid enters a cell, it binds to the androgen receptor. The steroid-receptor complex then translocates into the cell nucleus and acts as a transcription factor — directly influencing which genes are expressed and at what rate.
In skeletal muscle, this gene activation increases transcription of structural proteins involved in muscle fiber repair and hypertrophy — including myosin heavy chain and actin. The result is accelerated protein synthesis and a shift in the anabolic-to-catabolic balance toward net tissue growth. Anabolic steroids also reduce glucocorticoid (cortisol) signaling in muscle, meaning less breakdown during hard training or caloric deficit phases.
DHT Conversion and 5-Alpha Reductase
Testosterone converts to dihydrotestosterone (DHT) via the enzyme 5-alpha reductase in certain tissues: the scalp, prostate, and skin. DHT binds androgen receptors with significantly higher affinity than testosterone — making it far more potent in androgenic tissue. This conversion is why testosterone use carries risk of hair loss, acne, and prostate stimulation in sensitive individuals. Anabolic steroids that are already DHT derivatives — stanozolol, oxandrolone, drostanolone — bypass this conversion step and behave differently in androgenic tissue. Understanding which anabolic steroids convert to DHT and which do not is fundamental to risk assessment. See Hair Loss and DHT on Steroids for full detail.
Aromatization and Estradiol
Some anabolic steroids — testosterone being the primary example — convert to estradiol via the aromatase enzyme. Estradiol is not a toxin to be eliminated. It is a required hormone for bone mineral density, lipid regulation, cardiovascular protection, libido, and cognitive function. Managing aromatization means maintaining estradiol in a functional physiological range — not suppressing it. This distinction matters enormously for long-term health on cycle. For full context, see Estradiol Before Steroids and Estradiol on TRT.
Anabolic vs Androgenic Effects — What the Ratio Actually Means
Every anabolic steroid carries an anabolic-to-androgenic ratio — a number expressing its tissue-building versus masculinizing potency relative to testosterone, where testosterone = 100:100. These ratios were derived from animal bioassays measuring levator ani muscle growth versus prostate weight gain. They are useful as rough orientation but do not translate cleanly to human pharmacology. A ratio of 300:50 does not mean a compound causes six times more muscle growth at half the androgenic risk in clinical practice.
Anabolic effects include: increased muscle protein synthesis, improved nitrogen retention, enhanced red blood cell production, improved recovery from training stress, and IGF-1 upregulation. These are the properties that make anabolic steroids medically relevant in muscle-wasting diseases, anemia, and hypogonadism — and the effects that drive non-medical use in performance contexts.
Androgenic effects include: sebaceous gland stimulation causing acne, acceleration of male-pattern hair loss in genetically predisposed individuals, prostate tissue stimulation, virilization in biological females, and mood and behavioral changes. For compound-specific androgenic risk profiles, see Acne on Steroids, Gynecomastia Risk on Steroids, and Mood Changes on Steroids.
6 Key Physiological Effects of Anabolic Steroids
- 1
Increased Muscle Protein Synthesis
Anabolic steroids accelerate the rate at which muscle cells produce contractile proteins. This is the core mechanism behind muscle growth on cycle. Even at maintenance calories, anabolic steroids shift protein turnover toward net positive — more synthesis than breakdown. At caloric surplus, this effect is substantially amplified, which is why bulk-oriented cycles produce more muscle gain than deficit-phase protocols.
- 2
Nitrogen Retention
Muscle tissue is approximately 16% nitrogen by dry weight. A positive nitrogen balance — retaining more than is excreted — is the biochemical definition of an anabolic state. Anabolic steroids reliably shift nitrogen balance positive in muscle tissue, which correlates with muscle growth and reduced catabolism during caloric restriction or high-volume training blocks. Measuring nitrogen balance was historically the gold standard for confirming anabolic activity in early AAS research.
- 3
Erythropoiesis — Red Blood Cell Production
Many anabolic steroids stimulate erythropoiesis by increasing erythropoietin (EPO) output from the kidneys. More red blood cells means more oxygen delivery to working muscle — a meaningful advantage in endurance and high-volume training contexts. However, elevated red blood cell mass raises hematocrit and blood viscosity, increasing the risk of thromboembolic events. Monitoring hematocrit and hemoglobin on cycle is not optional. See Hematocrit & Hemoglobin.
- 4
IGF-1 Upregulation
Anabolic steroids increase hepatic insulin-like growth factor 1 (IGF-1) secretion. IGF-1 amplifies growth hormone signaling and exerts its own anabolic effects on muscle and connective tissue. This contributes to the synergistic muscle growth seen when anabolic steroids and growth hormone are combined. IGF-1 elevation also partially explains why connective tissue strain can occur even as strength increases rapidly — tendons and ligaments adapt more slowly than contractile tissue.
- 5
Anti-Glucocorticoid Effect
Anabolic steroids compete with cortisol for glucocorticoid receptor binding in muscle tissue. By partially blocking cortisol’s catabolic signaling, they reduce muscle breakdown during recovery, intense dieting, and high-volume training blocks. This is a significant mechanism behind the effectiveness of anabolic steroids during caloric deficit — where cortisol would otherwise accelerate lean mass loss disproportionately.
- 6
CNS and Neuromuscular Recovery
Anabolic steroids affect the central nervous system beyond muscle tissue. Elevated androgen signaling in the CNS is associated with increased aggression, drive, reduced perception of fatigue, and faster neuromuscular recovery between training sessions. These effects vary significantly by compound, dose, individual androgen receptor sensitivity, and baseline testosterone status. The behavioral effects of anabolic steroids are covered in detail in Mood Changes on Steroids.
Anabolic Steroids and Hormonal Suppression — The HPTA
One of the most clinically significant effects of anabolic steroids is suppression of the hypothalamic-pituitary-testicular axis (HPTA). The hypothalamus monitors circulating androgen levels and regulates gonadotropin-releasing hormone (GnRH) accordingly. When exogenous anabolic steroids are introduced, the hypothalamus detects supraphysiological androgens and reduces GnRH output. This suppresses LH (luteinizing hormone) and FSH (follicle-stimulating hormone) from the pituitary — and without LH, testicular testosterone production falls to near-zero.
The depth of suppression depends on the compound, dose, and duration. Some anabolic steroids — particularly 19-nor compounds like nandrolone — are deeply suppressive even at low doses due to progestin receptor activity alongside androgen receptor binding. Others, like oxandrolone at modest doses, produce comparatively milder suppression. But no anabolic steroid is non-suppressive at meaningful doses. Every exogenous androgen suppresses the HPTA to some degree. This is a pharmacological certainty, not a debatable point.
Suppression of endogenous testosterone during a cycle is the reason post-cycle therapy (PCT) exists — to pharmacologically restore HPTA function after the cycle ends. Recovery speed and completeness are highly individual and depend on cycle length, compound choice, and baseline testicular reserve. For full context, see the PCT hub.
Fertility and HPTA Suppression
Because FSH directly controls spermatogenesis in the testes, anabolic steroid use causes measurable reductions in sperm count — sometimes to azoospermia (zero viable sperm) at high doses or on prolonged cycles. For men actively trying to conceive, this is a critical consideration that must be evaluated before any AAS use. Recovery of fertility after anabolic steroids is possible but not guaranteed and varies substantially by individual and cycle history. See Fertility and Suppression on Steroids for a detailed breakdown.
Bloodwork Markers Affected by Anabolic Steroids
Any responsible discussion of anabolic steroids must include bloodwork. These compounds alter multiple organ systems simultaneously — and most of those changes are only visible through blood panels. Clinical symptoms of serious harm from anabolic steroids often appear late or not at all until damage is established. Bloodwork provides early-warning data that symptoms cannot.
Lipid Panel — HDL Suppression
Anabolic steroids reliably suppress HDL cholesterol and commonly raise LDL. The degree depends heavily on the compound: oral anabolic steroids — particularly 17-alpha-alkylated compounds like stanozolol — have dramatically worse lipid effects than injectable testosterone. Some 17aa oral AAS can drop HDL to single-digit levels within weeks. This is among the primary long-term cardiovascular risks of anabolic steroid use and one of the strongest arguments for aggressive pre-cycle baseline panels. See Lipid Panel: HDL, LDL, Triglycerides.
Liver Enzymes — AST, ALT, GGT
Oral anabolic steroids — specifically 17-alpha-alkylated compounds — resist first-pass liver metabolism, causing dose-dependent hepatotoxicity. AST and ALT elevations are expected and measurable. Monitoring liver markers before and during oral AAS use is non-negotiable. Injectable anabolic steroids generally carry far lower hepatotoxicity, though high-dose trenbolone and certain other injectables can still stress hepatic function. See Liver Markers: AST, ALT, GGT.
Hematocrit and Hemoglobin
Erythropoiesis stimulation on anabolic steroids raises hematocrit and hemoglobin. Hematocrit above 50–52% significantly increases blood viscosity and thromboembolism risk. Testosterone-based anabolic steroids tend to produce larger hematocrit elevations than DHT-derived compounds. This marker requires regular monitoring on any cycle involving testosterone or nandrolone-class compounds. See Hematocrit & Hemoglobin (CBC).
Hormonal Markers — LH, FSH, Testosterone, SHBG
On cycle, LH and FSH are suppressed to near-zero. Total testosterone reads supraphysiologically high if a testosterone-based AAS is used; reads low if a non-testosterone AAS is used without a testosterone base. SHBG is commonly lowered by anabolic steroids, affecting free testosterone calculations. For interpretation context, see Total vs Free Testosterone, SHBG Explained, and TRT Bloodwork.
Baseline bloodwork before anabolic steroid use is not optional for harm reduction — it is the foundation. Without knowing your pre-cycle lipids, liver enzymes, hematocrit, testosterone, and kidney markers, you have no reference point for interpreting any change that occurs during use. See Blood Tests Before Steroids: 7 Markers to Check.
5 Common Mistakes When Researching Anabolic Steroids
- Mistake
Skipping Baseline Bloodwork
Researching anabolic steroids without establishing your baseline hormonal, lipid, liver, and hematological values means you have no reference point for interpreting any change that occurs. Baseline bloodwork is not a precaution — it is the minimum data requirement for harm reduction. See Blood Tests Before Steroids.
- Mistake
Treating Anabolic-to-Androgenic Ratios as Predictive
The anabolic-to-androgenic ratio is a laboratory measurement from rat bioassays. It does not map cleanly to human side effect profiles. Using ratios as the primary risk assessment tool for anabolic steroids leads to systematically poor compound selection decisions.
- Mistake
Treating Estradiol as an Enemy
Many first-time researchers assume estrogen must be fully suppressed during anabolic steroid use. This is incorrect and dangerous. Estradiol is required for cardiovascular health, bone density, libido, and cognitive function. Aggressive estrogen suppression on cycle causes significant harm. See Estradiol Before Steroids.
- Mistake
Underestimating HPTA Suppression
Every anabolic steroid suppresses the HPTA at meaningful doses. Assuming a compound is mild or non-suppressive based on forum consensus or marketing language is a reliable path to prolonged hypogonadism after a cycle ends. HPTA recovery is not guaranteed and is not always fast, particularly after long cycles or stacks involving 19-nor compounds.
- Mistake
Using Anabolic Steroids Before Optimizing Training and Nutrition
Anabolic steroids amplify the training stimulus — they do not replace it. Using them without a consistent, structured training program and adequate protein intake produces significantly less result at identical risk. The Training hub and Nutrition hub cover the foundations that should precede any AAS research.
Authoritative Sources on Anabolic Steroids
- NCBI StatPearls — Anabolic Steroids: Pharmacology, Classification, Monitoring, and Adverse Effects
- PubMed — Effects of Supraphysiologic Doses of Testosterone on Muscle Size and Strength
- PubMed — Cardiovascular Toxicity of Illicit Anabolic-Androgenic Steroid Use
- PubMed — Effects of Androgenic-Anabolic Steroids on Apolipoproteins and Lipoprotein(a)
- PubMed — Adverse Health Consequences of Performance-Enhancing Drugs: Endocrine Society Scientific Statement
- MedlinePlus — Anabolic Steroids: Health Risks Overview
What You Need to Know About Anabolic Steroids Before Going Further
Anabolic steroids are synthetic testosterone derivatives that activate androgen receptors, driving muscle protein synthesis, nitrogen retention, and red blood cell production. They simultaneously suppress the HPTA, degrade lipid profiles, stress the liver — particularly with oral 17-alpha-alkylated compounds — raise hematocrit, and alter estradiol. All of these effects are measurable and, with proper bloodwork protocols, manageable.
The biology of anabolic steroids is well-documented in the research literature. The risks are real, quantifiable, and highly individual. The harm-reduction framework rests on one non-negotiable requirement: know your baseline, monitor on cycle, and understand what the numbers mean before acting on them.
Continue through the Steroids hub for compound-specific education. Use the resources below for the adjacent topics that anabolic steroid use directly affects.
This article is published for educational and harm-reduction purposes only. Anabolic steroids are controlled substances in many jurisdictions. Nothing written here constitutes medical advice, a recommendation to use any compound, or guidance on sourcing or legal compliance.
All content on MuscleScience.org is produced by writers working under pseudonyms for editorial independence. Author photographs are stylized portraits, not real images of the writers. See our About page for full editorial disclosure.
We do not sell. We do not supply. We educate.


